Background: In Hospital Medicine, change isn’t coming—it’s already here. Transition is perhaps the only constant in this field. Whether it’s billing models, quality metrics, staffing, reimbursements, or even contracts, evolution is inevitable. A significant shift occurred when Nurse Practitioners (NP) and Physician Assistants (PAs), collectively referred to as Advanced Practice Providers (APPs), joined hospitalist groups. Over the years, these APPs have firmly established themselves as hospitalists, with APPs now present in 79.8% of Hospital Medicine Groups (HMGs) nationwide [1]. Our academic Hospital Medicine Group eliminated its APP positions as part of a policy shift enacted by our partner hospital. We studied the impact of transitioning from physician-APP teams to physician-only teams on Length of Stay (LOS).
Methods: Our group staffs five resident teams, eight direct care teams, and three physician-only transplant teams at a 1000-bed, safety net academic medical center. 6 out of 8 direct care teams operated under a dyad model until February 2025, during which APPs provided shared services under the supervision of a collaborating hospitalist. Each team handled an average of 15 encounters per day, with physicians and APPs serving as primary hospitalists for roughly half of the team. APP role elimination began in February 2025, and by the end of August 2025, all direct care teams had transitioned to physician-only teams. We compared Average Length of Stay (ALOS), Case Mix Index (CMI), mortality, and 30-day readmission rates in the baseline (March-August 2024) and intervention (March-August 2025) periods. Means were compared using Welch’s t-test, while the chi-square test was used for proportions. We also generated a control chart of Observed-to-Expected (O/E) LOS for January and September 2025.
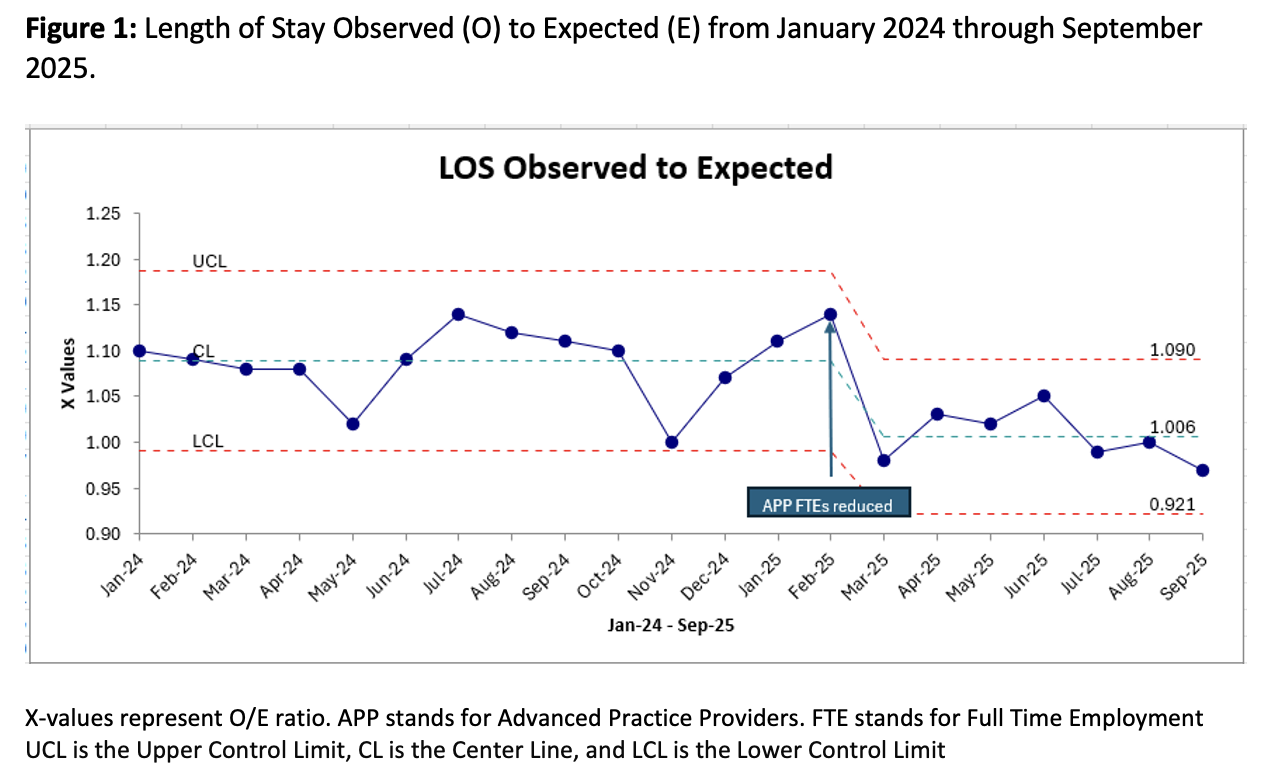
Results: ALOS decreased from 7.9 days during baseline (n=4061) to 7.3 days during intervention (n=4062) period (p=0.0017). CMI increased slightly from 1.72 to 1.74, while the 30-day readmission rate (17.42% versus, p-value 0.71) and mortality (0.84% versus 0.78%, p-value 0.76) were unchanged. The control chart (Figure 1) shows a non-random decline in O/E LOS starting in March 2025.
Conclusions: The Transition from a physician-APP dyad model to physician-only teams was associated with a reduction in LOS at our hospital. This may be due to improved efficiency and reduced decision-making time in the physician-only model. Further research is needed to determine whether a dyad model in which APPs function as physician extenders rather than primary hospitalists for half the team will affect LOS differently.