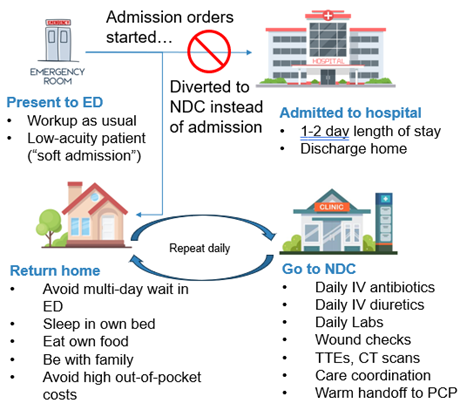
Background: U.S. hospitals are facing unprecedented strain: ED boarding times are at an all-time high and a national hospital bed shortage is predicted as early as 2032. The leading hospital-substitution model, Hospital at Home, faces financial uncertainty as the waiver allowing its reimbursement expired in September 2025 and now only exists through a continuing resolution that expires January 2026. Scalable alternatives are urgently needed. A prior observational study established the NDC as a practical outpatient alternative to hospitalization by offering scheduled services historically rendered in a hospital setting: multi-day courses of IV antibiotics and diuretics, daily STAT labs and clinician re-evaluation, specialist consultation, and rapid access to advanced imaging and cardiodiagnostics, as examples (Exhibit 1). This study reports the first-ever randomized controlled trial (RCT) of an NDC model.
Methods: We conducted a 6-month pragmatic parallel-group RCT of adults presenting to the emergency department (ED) who were in the process of being admitted (admission orders were underway). An automated EHR rule flagged eligible patients, and ED physicians were prompted to reverse the admission decision if clinically appropriate. This created a randomized encouragement design in which treatment patients had access to the NDC while control patients did not. The primary outcome was days alive and out of hospital (DAOH) at 30 days from the index ED visit. Secondary outcomes were all-cause 30-day hospital readmissions and total cost of care (until discharged from the hospital or NDC care) from health system financial records. The primary analysis was pre-registered on clinicaltrials.gov (NCT06526884) and used instrumental variable regressions, leveraging randomization as the instrument for treatment received.
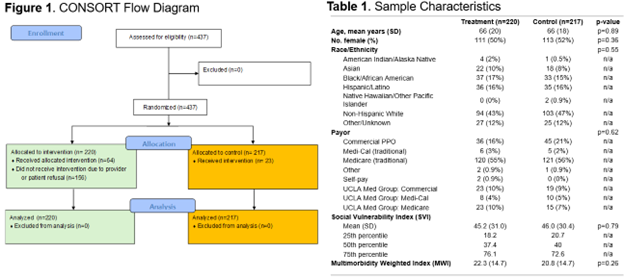
Results: There were 437 eligible patients who were randomized, yielding 220 treatment patients and 217 control patients (Exhibit 2). The instrumental variable analysis showed that NDC treatment resulted in 4.4 more DAOH at 30 days (95% CI 0.50–9.31; p=0.028) per referral compared to usual admission. Thirty-day readmissions were similar (4.7% vs 4.1%; p=0.46). Actual episode expenditures averaged $404 per NDC episode, compared with $13,354 for standard hospital care—representing $12,950 in avoided expenditures per NDC referral. NDC patients had their first post-ED follow-up an average of 20 hours from ED discharge and went home between NDC visits.
Conclusions: In the first randomized trial of a high-acuity clinic alternative to hospitalization, the NDC model produced significantly more days alive and out of the hospital and dramatically lower costs, without increased readmissions. This infrastructure-light, clinic-based model offers one of the most scalable, financially viable, and clinically robust hospital-substitution strategies to date. The NDC represents a transformative opportunity for health systems seeking to relieve capacity strain while delivering high-value acute care.