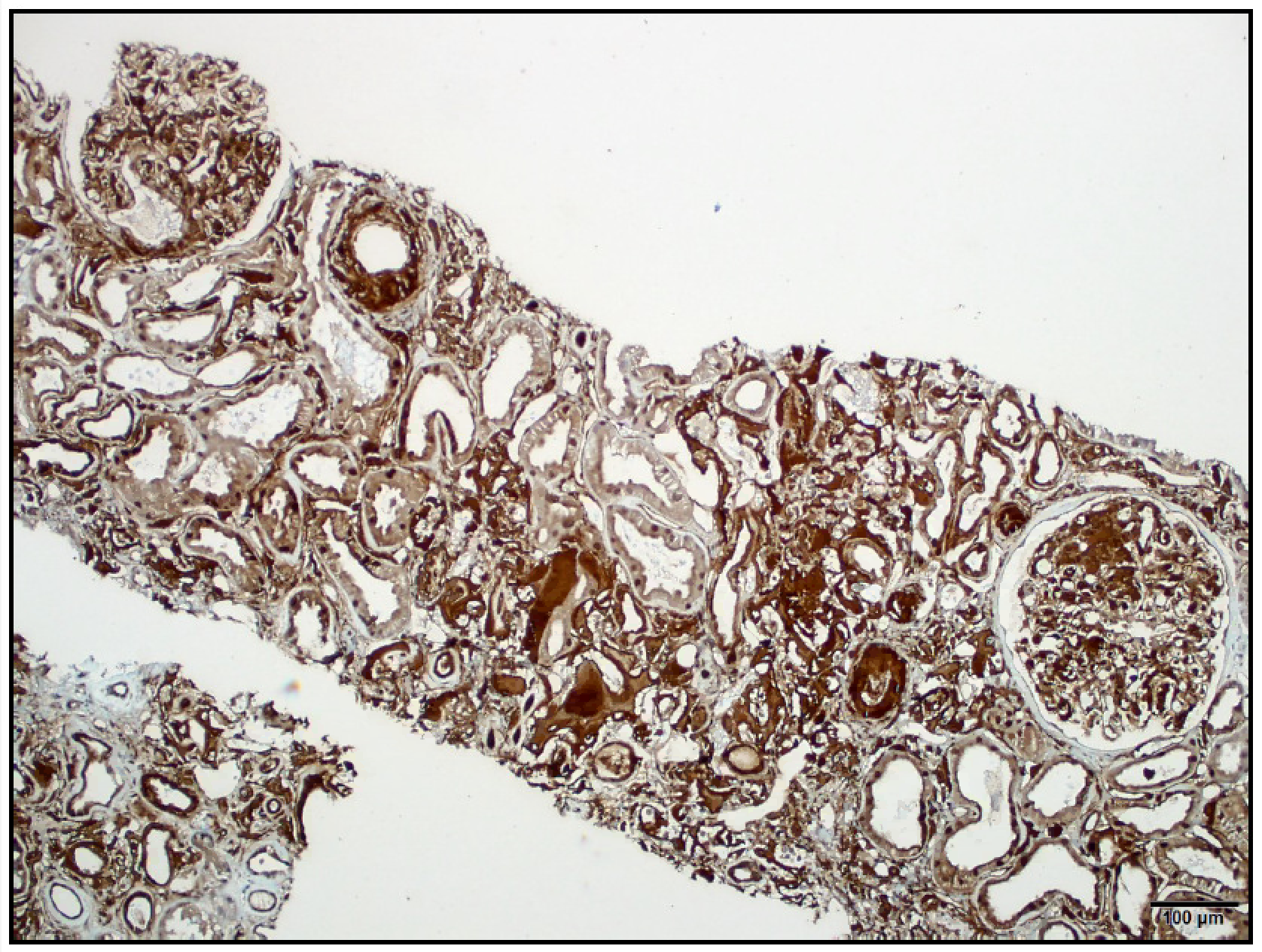
Case Presentation: A 64-year-old Pakistani man was referred to nephrology clinic for evaluation of progressive kidney disease. Relevant medical history included well-controlled type 2 diabetes mellitus, gout and hypertension. Six months prior to presentation his serum creatinine level was 2.9 mg/dL (eGFR 22 ml/min per 1.73m2), patient had been asymptomatic and had well-controlled co-morbidities without known complications. Since that time, his kidney function had worsened with a creatinine level of 3.56 mg/dL (eGFR 17 ml/min/1.73m2) on presentation. The patient’s sister and mother had been diagnosed with chronic kidney disease (CKD) of unknown etiology back in Pakistan. Further studies revealed no active urinary sediment and non-nephrotic range proteinuria with a urine protein-to-creatinine ratio 0.32 gm. Renal ultrasound showed increased echogenicity of renal cortex without nephrolithiasis or hydronephrosis. Due to worsening kidney function of unclear etiology, patient underwent kidney biopsy that revealed abundant interstitial and glomerular amyloid deposits, negative for light and heavy chains, but strongly positive immunohistochemistry for leukocyte chemotactic factor 2 (LECT2) in interstitial, glomerular and arteriolar deposits; all of these findings on a background of CKD compatible with hypertensive nephrosclerosis. Features consistent with LECT2 renal amyloidosis.
Discussion: Amyloidosis resulting from leukocyte cell-derived chemotactic factor 2 (ALECT2) is an emerging type of amyloidosis, first described in 2008, causing almost 50% of cases of renal amyloidosis in the Southwest region of the United States and is still thought to be underdiagnosed. Most patients are elderly (median age 65 years) present with CKD, bland urinary sediment and non-nephrotic proteinuria. Concurrent hypertension and diabetes is common, with up to 26.4% of cases presenting with underlying kidney disease, as was the case of our patient. Overall survival is better than with other types of amyloidosis, likely due to the rarity of cardiac involvement, nevertheless renal prognosis is guarded since most patients inevitably progress to end stage renal disease (ESRD). No definite therapy is currently available and further research is needed to better understand the pathogenesis of diseases. While LECT2 is traditionally associated to cell growth or damage it does not seem to be an over expression of ALECT2 genes that causes deposition in the kidney. Establishing a definite and accurate diagnosis is critical for the clinician as this can prevent starting ineffective and potentially harmful treatment. Previous reports have described patients being mistakenly treated for immunoglobulin light chain amyloidosis and receiving chemotherapy for presumed plasma cell dyscrasias, which provided no benefit and did not prevent the final outcome of inevitable progression to ESRD only increasing cost and potential risk for iatrogenic harm.
Conclusions: 1. ALECT2 nephropathy is an emerging cause of renal disease2. Patients in whom ALECT2 nephropathy is suspected must undergo definite diagnosis and readily identified in order to avoid potentially harmful unnecessary treatment