Background: Ambulatory care sensitive conditions (ACSCs) are a set of diagnoses that if not recognized and addressed properly in the ambulatory setting can lead to preventable hospitalizations. People experiencing homelessness (PEH) often have barriers to access of ambulatory care services and chronic disease self-management. These place them at high risk for having ACSCs, and contribute to high rates of acute care utilization. Homeless healthcare teams can diagnose and treat ACSCs among PEH. However, the prevalence of ACSCs among PEH treated by homeless healthcare teams has not been described in the literature. We aimed to describe the experience of a Los Angeles County homeless healthcare team with ACSCs and determine if certain sociodemographic subgroups experienced higher rates of ACSCs.
Methods: We performed a cross-sectional analysis of adult patients aged 18-years or older treated by the Homeless Healthcare Collaborative (HHC), UCLA Health’s field-based homeless healthcare team, between January 2022 and August 2023. Data for this study were based on electronic health records (EHR). The outcome of interest was based on ICD-10 codes and included the diagnosis of one or more of the following ACSCs during a clinical encounter: anemia, angina, asthma, cellulitis, congestive heart failure, chronic obstructive pulmonary disease, dental condition, diabetes mellitus, epilepsy, gangrene, gastroenteritis, hypertension, lower extremity ulcer, pneumonia, and urinary tract infection. Sociodemographic factors including age, gender identity and race or ethnicity for each patient were also extracted from the EHR. We performed descriptive statistics of the cohort. Factors associated with ASCS were evaluated using multi-level multivariable logistic regression model which accounted for repeat visits for some patients.
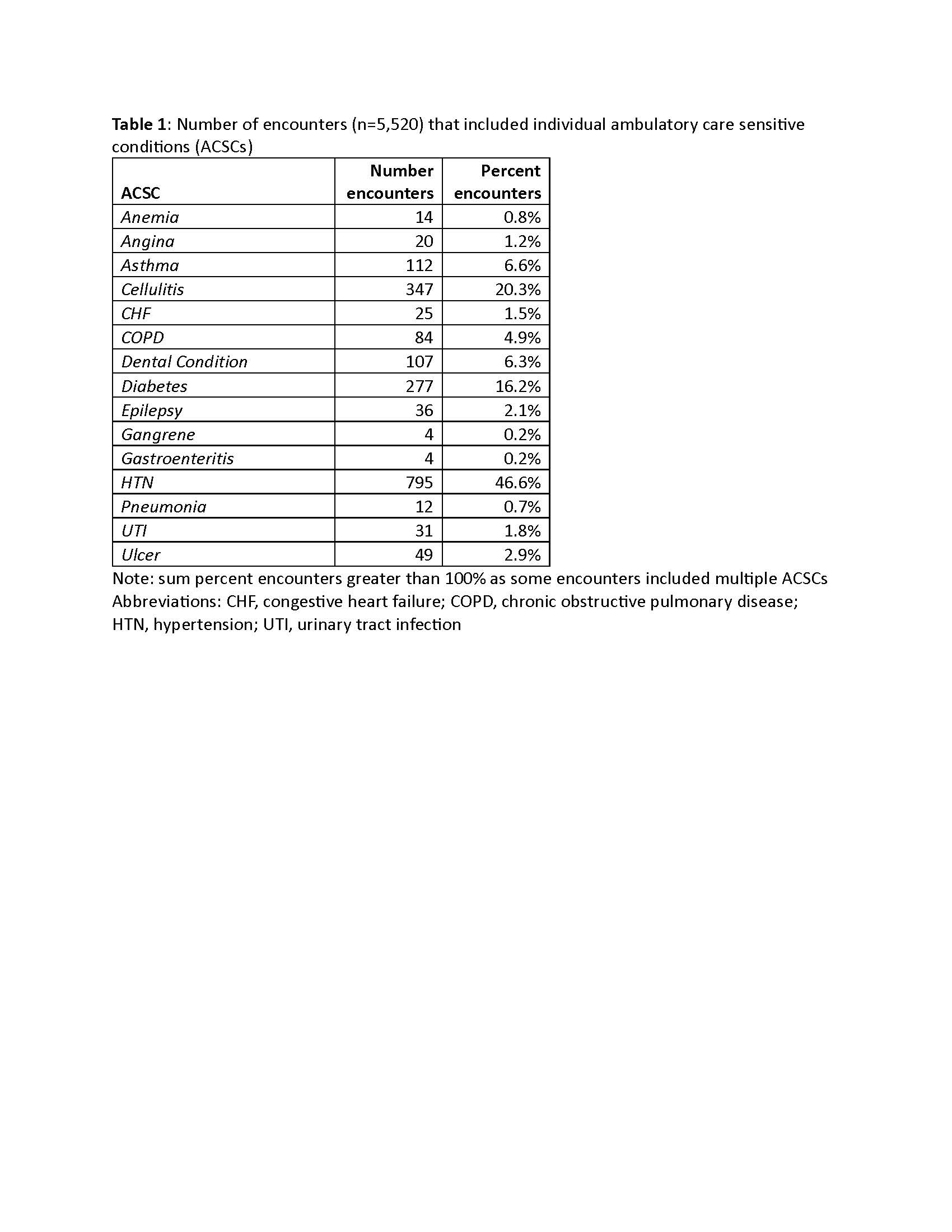
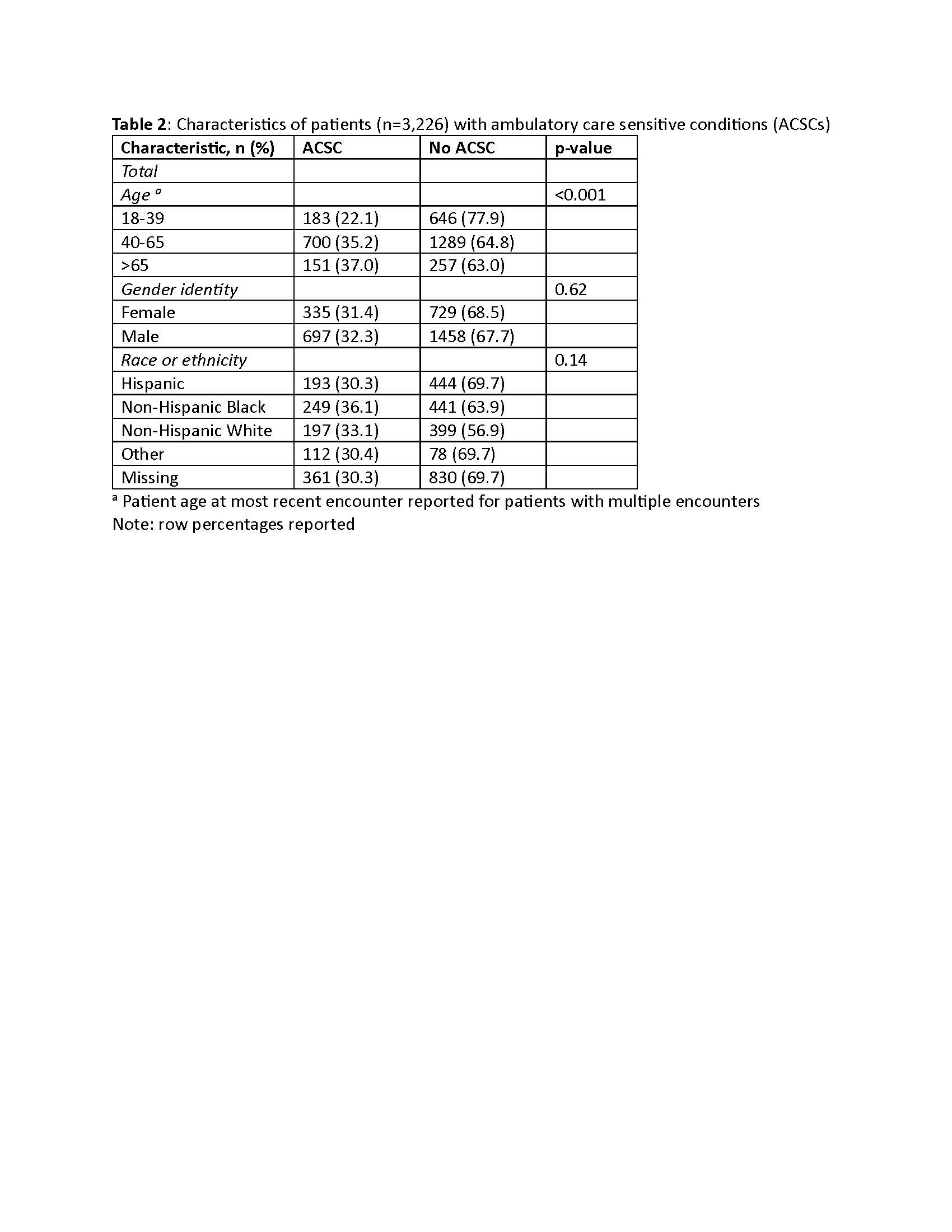
Results: Overall, HHC performed 5,520 encounters among 3,226 unique patients. Among unique patients, 33.0% were female, 25.7% were 18-39, 61.7% were 40-65, and 12.7% were over 65 years of age (age at date of last encounter for patients with multiple visits). Race and ethnicity of patients included: 19.8% Hispanic, 21.4% non-Hispanic Black (NHB), and 18.5% non-Hispanic White (NHW) (35.7% had unknown race). The prevalence of ACSC across all encounters was 30.9% and the most common ACSCs encountered were hypertension (46.6%), cellulitis (20.3%) and diabetes (16.2%) (Table 1). ASCSs were more common among patients older than 65 (37.0% among those >65 years of age vs. 22.1% among those 18-39 years of age; p<.001) (Table 2). Based on multivariable analyses, the odds of having an encounter with an ACSC increased with age (adjusted OR 1.16 per age increase by 10 years, 95% CI 1.09, 1.25; p< 0.001) and differed by race and ethnicity with NHB having higher odds of ACSCs as compared to NHW patients (adjusted OR 1.27, 95% CI 1.01, 1.61; p=0.042).
Conclusions: ACSCs were commonly encountered by our LA-based street medicine team, with nearly a third of patients and a third of encounters involving an ACSC. Older and NHB patients had greater odds of having an encounter for an ACSC. We suspect the high prevalence of ACSCs among patients treated by our homeless healthcare team is similar to the experience of others. Therefore, homeless healthcare has the potential to prevent hospitalizations for this vulnerable population by providing high-quality ambulatory care. Further evaluation is ongoing to determine if encounters with HHC are associated with decreased acute care utilization.