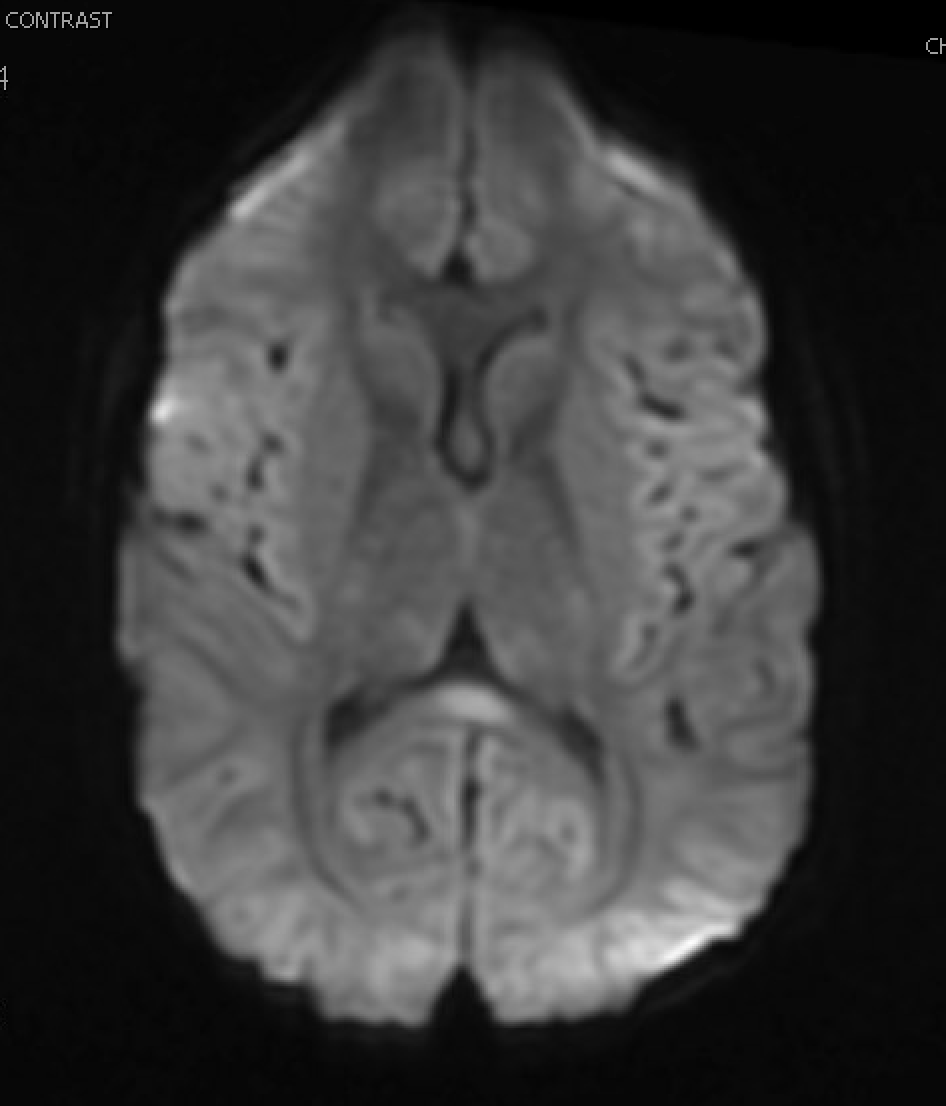
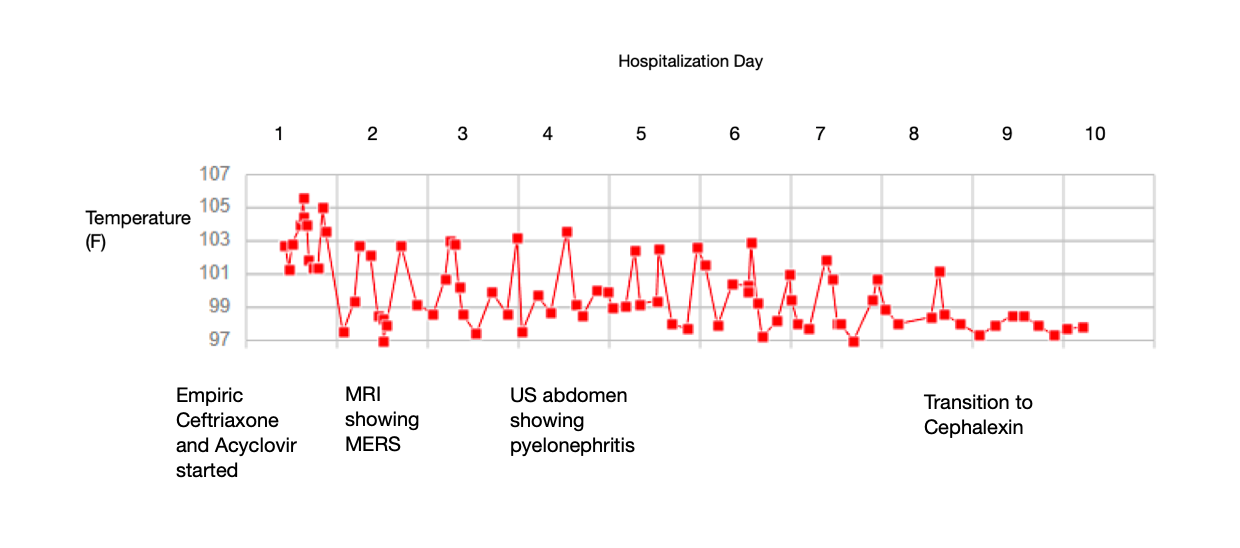
Case Presentation: MERS is a radiological-clinical diagnosis with distinct MRI findings and neurological symptoms often associated with an infectious process. Clinical symptoms can include headache, vision changes, delirium, abnormal speech, and seizures. Brain MRI classically demonstrates symmetric lesions in the splenium of the corpus callosum with restricted diffusion. MERS is generally self-limiting and often occurs in the setting of viral infection. It is rarely reported to have association with pyelonephritis. We present an 8-year-old male presenting with MERS, subsequently discovered to have pyelonephritis.An 8-year-old previously healthy male presented with 2 days of headache, vomiting, and fever to 104F. In the ED, he was noted to be lethargic, intermixed with periods of incoherent speech. Initial imaging studies included head CT and chest X-ray, both normal. Labs showed mild leukocytosis (11,300) and mild hyponatremia (134). CSF studies showed negative gram stain, meningitis-encephalitis panel, and ultimately negative culture. The patient was treated with Ceftriaxone empirically. There was no report of dysuria or frequency; therefore, urinalysis and urine culture were only obtained after initiation of antibiotics and showed no evidence of infection. The patient underwent brain MRI, which revealed a lesion in the corpus callosum. Due to significant abdominal tenderness on exam, an ultrasound was obtained and showed left pyelonephritis. Pain and mental status improved with antibiotic therapy. He was discharged on Cephalexin with complete resolution of neurological symptoms by the end of the treatment course.
Discussion: The exact pathophysiology of MERS is unknown but may be due to cascades of various cytokines, leading to an influx of water into astrocytes and neurons, resulting in cytotoxic edema. This mainly affects the corpus callosum but can extend to other white matter. The wide spectrum of neurological symptoms reported represent the inherent characteristic of the corpus callosum as the biggest nerve fiber bundle, with projections to multiple areas of the brain. Our patient was unique in that delirium and fever were his initial presenting symptoms, with onset of abdominal pain after hospital admission. Classic symptoms of dysuria and frequency were not seen, and there was no pyuria or leukocyte esterase on urinalysis. The only clue to his pyelonephritis diagnosis was abdominal pain, which was seen on renal ultrasound. MERS often abates with supportive care for viral illnesses or treatment of the underlying bacterial infection, so it is important to elicit this early in the clinical course. So far, all reported pediatric patients with MERS, including ours, had rapid resolution within 1 month of adequate treatment.
Conclusions: Fever and altered mental status often necessitate a thorough neurological workup but as this case demonstrates, MERS may be a presenting symptom for extra-neurological etiologies like acute pyelonephritis. In cases of MERS without apparent viral etiology, pyelonephritis should be strongly considered.