
Case Presentation:
A 31‐year‐old white man with a history of schizoaffective disorder, nonadherent to therapy, was brought to the emergency department for paranoia. The patient had developed a fear of eating, initially of most protein sources and subsequently of fruits and vegetables. His diet consisted of a case of water, a loaf of Italian bread, and grits. He had an 88‐pound weight loss over the 15 months prior to presentation following dietary changes. He complained of occasional blood on toilet paper when straining but no abdominal pain. He also felt weak and noted his skin had changed color. He denied any blood loss, trauma, or recent surgery. Physical exam revealed normal vital signs, dry mucous membranes, pale conjunctivae, icteric sclerae and poor dentition. Abdominal striae, diffuse perifollicular hemorrhage, hyperkeratosis with corkscrew hair, and localized ecchymosis over the left calf were present. Initial laboratory studies demonstrated sodium 114 mEq/L, creatinine 0.8 mg/dL, and hemoglobin 5 g/dL with normal red blood cell indices. In addition to packed red blood cell transfusion, he received a 1‐g ascorbic acid load and then 500 mg daily for his scurvy and a psychiatric consultation for his paranoia with underlying schizoaffective disorder.
Discussion:
Scurvy, a disease caused by ascorbic acid (vitamin C) deficiency, is found in alcoholics, the isolated elderly, and the mentally ill in modern industrialized nations. Symptoms of scurvy include bleeding and bruising easily, hair and tooth loss, and joint pain and swelling. The combination of follicular hyperkeratosis and perifollicular hemorrhage is pathognomonic and occurs early in the disease. Such symptoms appear to be related to the weakening of blood vessels, connective tissue, and bone, which all contain collagen. The diagnosis of scurvy is mainly clinical, with laboratory values playing a confirmatory role. The response to replacement therapy is rapid and also aids in establishing the diagnosis. The recommended dietary allowance for vitamin C is 60–95 mg for adults.

Bilateral lower extremities demonstrating hyperkeratosis and peri‐follicular hemorrhage.
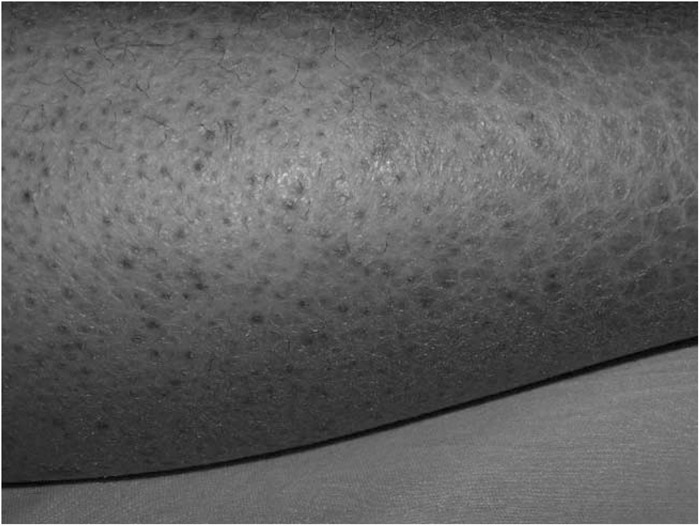
Anterior leg demonstrating corkscrew hair, perifollicular hemorrhage, and hyperkeratosis.
Conclusions:
The purpose of reporting this case is to increase awareness about the importance of a thorough history and physical exam. Often neglected, a dietary history is quickly and easily taken and is essential to making the diagnosis. Hospitalists should be aware of those patients at risk and, although it is rare, include scurvy in the differential diagnosis because it is easily cured and certainly fatal if unrecognized and left untreated. Clinical acumen and knowledge of rare diseases like scurvy can decrease the cost of hospitalization. Length of stay can be minimized by limiting unnecessary testing and consultations.
Disclosures:
H. Sayed ‐ none; S. Coutinho McAllister ‐ Merck, speakers bureau; P. Stone ‐none