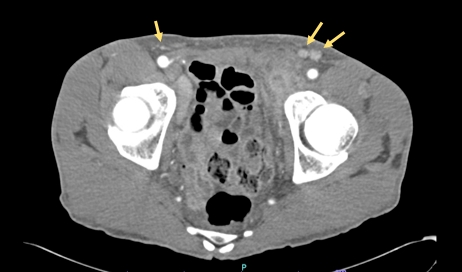
Case Presentation: A 55-year-old male with a history of hypertension and bipolar disorder presented with abdominal and groin pain, and unintentional 40lb weight loss over the past 4 months. Furthermore he reported fevers, chills, hematuria, and dysuria. On physical exam he had right upper quadrant abdominal tenderness, bilateral hard and immobile inguinal lymph nodes, and a well-circumscribed 1 cm erythematous ulcer with a smooth base on the glans penis. Initial laboratory evaluation revealed ALP of 1166, ALT of 668, AST of 227. In addition ESR was elevated to 113 and CRP of 1.1. CT imaging demonstrated pelvic lymphadenopathy up to 2.3 cm with enlarged retroperitoneal lymph nodes, while MRI of the abdomen did not show evidence of cirrhosis. Additional workup was significant for positive anti-mitochondrial antibody, anti-smooth muscle antibody, Treponema pallidum antibody, and rapid plasma reagin titer 1:32. Excisional biopsy of a right inguinal lymph node was performed and pathology revealed syphilitic lymphadenitis. The patient was treated for secondary syphilis with intramuscular penicillin G benzathine and liver enzymes downtrended. He was ultimately treated for secondary and latent syphilis with doxycycline 100mg twice a day for 4 weeks, as he had a penicillin allergy and refused desensitization. At 1-month follow-up, he reported significant improvement.
Discussion: Syphilis is a systemic illness caused by the gram-negative spirochete Treponema pallidum. During the primary stage, a painless sore known as a chancre develops in the genital area. Progression of untreated primary disease leads to secondary syphilis, where the infection can spread throughout the body and cause non-specific symptoms such as a rash, weight loss, fatigue, lymphadenopathy, and headaches, similar to our patient.Syphilitic hepatitis is a rare complication in which patients present with symptoms of hepatitis and marked elevation in alkaline phosphatase levels. In 2004, four diagnostic criteria of syphilitic hepatitis were proposed, including (1) abnormal liver enzyme levels; (2) serologic evidence of syphilis; (3) exclusion of other causes of liver disease; (4) liver enzyme levels returning to normal after appropriate antimicrobial therapy. Penicillin is the treatment of choice for syphilis. Our patient met all of the above criteria after extensive workup ruled out other causes of hepatitis and his liver enzymes normalized after treatment. Interestingly, as with our patient, anti-mitochondrial antibody and anti-smooth muscle antibody can also be present because of cross-reactivity between these antibodies and T. pallidum membrane structures.
Conclusions: Syphilitic hepatitis is an uncommon complication of syphilis. Our patient displayed a characteristic chancre suggestive of T. pallidum infection. We report this case to emphasize the consideration of syphilitic hepatitis as a diagnosis when at-risk patients present with lymphadenopathy and transaminitis, as appropriate antibiotic treatment leads to prompt resolution of symptoms.