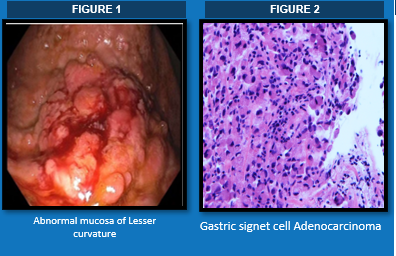
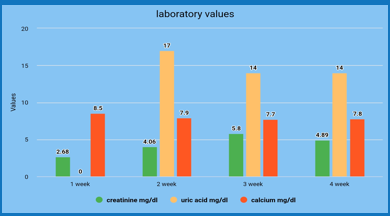
Case Presentation: Tumor lysis syndrome (TLS) is a potentially fatal complication usually seen in rapidly proliferating and chemo-sensitive malignancies like acute leukemia and lymphomas. (1-3) It is termed “spontaneous” (STLS) when TLS occurs without prior chemotherapy. (1) The incidence of STLS in solid tumors is infrequent/rare and can be fatal without early recognition and aggressive treatment.76-year-old Caucasian male admitted to the hospital with 2-weeks history of abdominal distention associated with dyspnea on exertion and subjective weight gain of 29 pounds in two months. The patient denied fever, chills , abdominal pain, nausea, vomiting, diarrhea, hematemesis, or hematochezia. His past medical history is significant for hypertension, CKD stage 2 and HFpEF. The patient had a ten-pack-year smoking history and a family history of heart disease of unknown etiology in his father. Pertinent physical examination reveals a firm and distended abdomen with a positive fluid wave sign, no signs of guarding or rebound tenderness. Creatinine 2.68mg/dl, Potassium 4.4mmol/L, and Calcium 8.5mg/dl. All other systemic examinations were grossly normal. Over the course of first week, paracentesis was performed, about 6L of ascitic fluid was drained that revealed tumor cells of adenocarcinoma of unclear origin. Tumor markers carcinoembryonic antigen, cancer antigen 19.9, prostate specific antigen all were negative. During the hospital course, the patient developed acute on chronic renal failure with marked hyperuricemia and hypocalcemia. Significant lab findings were Creatinine 4.83mg/dl, Potassium 4.5mmol/Calcium 7.9mg/dl, and Uric acid 17mg/dl. Subsequently, a Gastro-Esophago-Duodenoscopy with Endoscopic Ultrasound ( EGD-EUS) was performed, which identified a mucosa with localized granularity and a nodular mass on the lesser curvature of the stomach. Fine needle aspiration was performed, which showed a signet ring cell adenocarcinoma of gastric origin. The patient was treated with Rasburicase and Allopurinol for elevated uric acid and was also initiated on hemodialysis. However, the patient deteriorated with development of multi-organ failure and was unable to tolerate hemodialysis. The patient opted for comfort measures and passed away in his fourth week of admission.
Discussion: TLS is an oncologic emergency, that occurs when large amounts of tumor cells breakdown, with release of their cell contents into the blood circulation.[1,2] This results in metabolic abnormalities of hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia and acute renal failure which may further lead to cardiac arrhythmias or seizures.[3] Cairo-Bishop classification, the most used criteria to diagnose TLS, requires two laboratory and one clinical complication from the above findings to confirm it. Our patient had hyperuricemia and hypocalcemia, followed by acute renal failure as a clinical complication. Our case is a rare presentation of spontaneous tumor lysis syndrome (STLS) in a patient with gastric adenocarcinoma. Our literature review revealed 9 cases of TLS reported in the context of gastric adenocarcinoma, out of which only four correspond to spontaneous TLS. Our case would be the fifth reported case of STLS from gastric adenocarcinoma. (4,5)
Conclusions: Our hope is to increase awareness about the potential development of STLS in gastric adenocarcinoma and other solid tumors. Limited case reports and a low incidence rate makes it rare which can lead to the diagnosis being missed or delay.