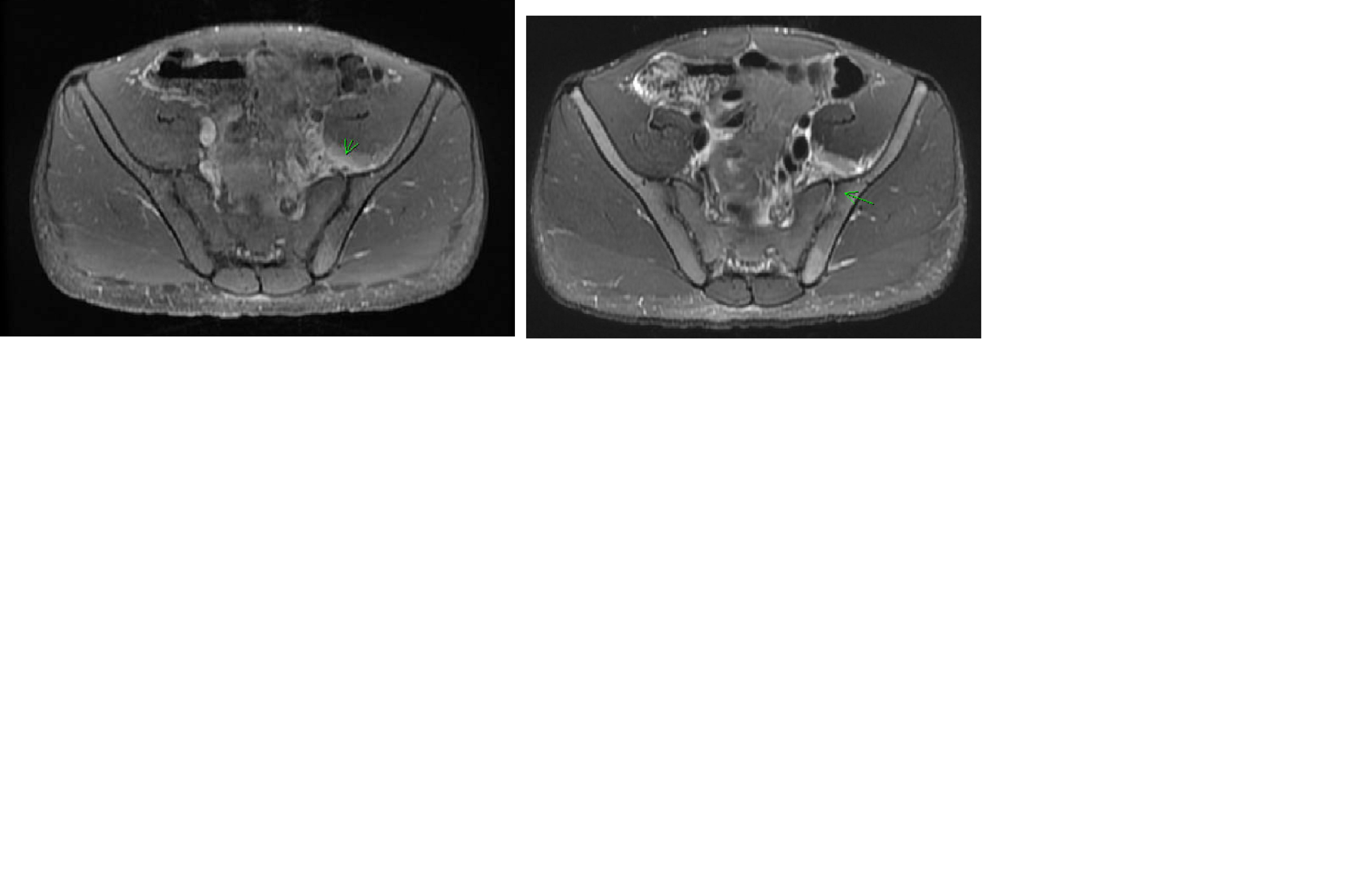
Case Presentation: Here is a case report that describes an immunized immunocompetent 17-year-old male who presented with acute onset sharp migratory poly-articular pain and swelling as a solitary complaint that began in the left hip and right wrist associated with night sweats and difficult ambulation. Fever and other systemic symptoms were absent. Upon initial work-up, he had significantly elevated inflammatory markers with CRP of 19 and ESR of 120 but a normal WBC of 9.4 with 68% neutrophils. Infectious and rheumatologic work-up was done. Blood culture at 20 hours showed growth of beta lactamase negative Haemophilus influenzae (Hi). Additional tests were remarkable for borderline low complement C4 level, positive anti-histone antibody with negative ANA titre but negative HIV serology, and normal immunoglobulin panel and other complement levels. Imaging included MRI of sacrum which showed unilateral left-sided sacroiliitis with bone marrow edema of left iliac bone and MRI right hand with diffuse subcutaneous tissue edema. The patient was diagnosed with bacteremia and poly-articular (left sacroiliac, right hand, bilateral shoulder, and right ankle) septic arthritis. Aspirate obtained from the left sacroiliac joint after antibiotic initiation only grew Staphylococcus epidermis that was considered a contaminant. The patient underwent aggressive treatment with parenteral antibiotics and completed two months of extensive regimen (including oral) to achieve complete remission.
Discussion: Isolation of Hi as a causative pathogen for invasive septic arthritis and bacteremia in an immunocompetent individual has been unusual in the post-vaccination era. The incidence of invasive disease by H influenzae type b (Hib) has declined substantially since the advent of vaccines per data from Centers for Disease Control and Prevention (CDC). However, an increase in incidence of ~ 16% has been noticed in invasive disease by non-Hib strains particularly nontypeable Hi (NTHi) and non-b encapsulated serotype a in the United States from 2009 to 2015. While NTHi may cause invasive disease in all age groups, they are supposed to be less virulent and manifest predominantly in infants and elderly population. Additionally, H influenzae affecting multiple joints is an uncommon occurrence. Due to this rarity in clinical presentation, we felt this case report will provide additional insight on Hi virulent strains, its unique presentation and management strategies particularly in musculoskeletal infections.
Conclusions: Vaccine preventable causes of infections may often get overlooked, particularly in the immunized population. This case report is one of the very few cases available in literature that describes H influenzae invasive infection in a healthy immunized child with no predisposing risk factors and with his unusual presentation and gives an account of management strategies used. Due to paucity of such cases and under-studied pathogenicity of non-capsulated strain, management strategies remain limited.