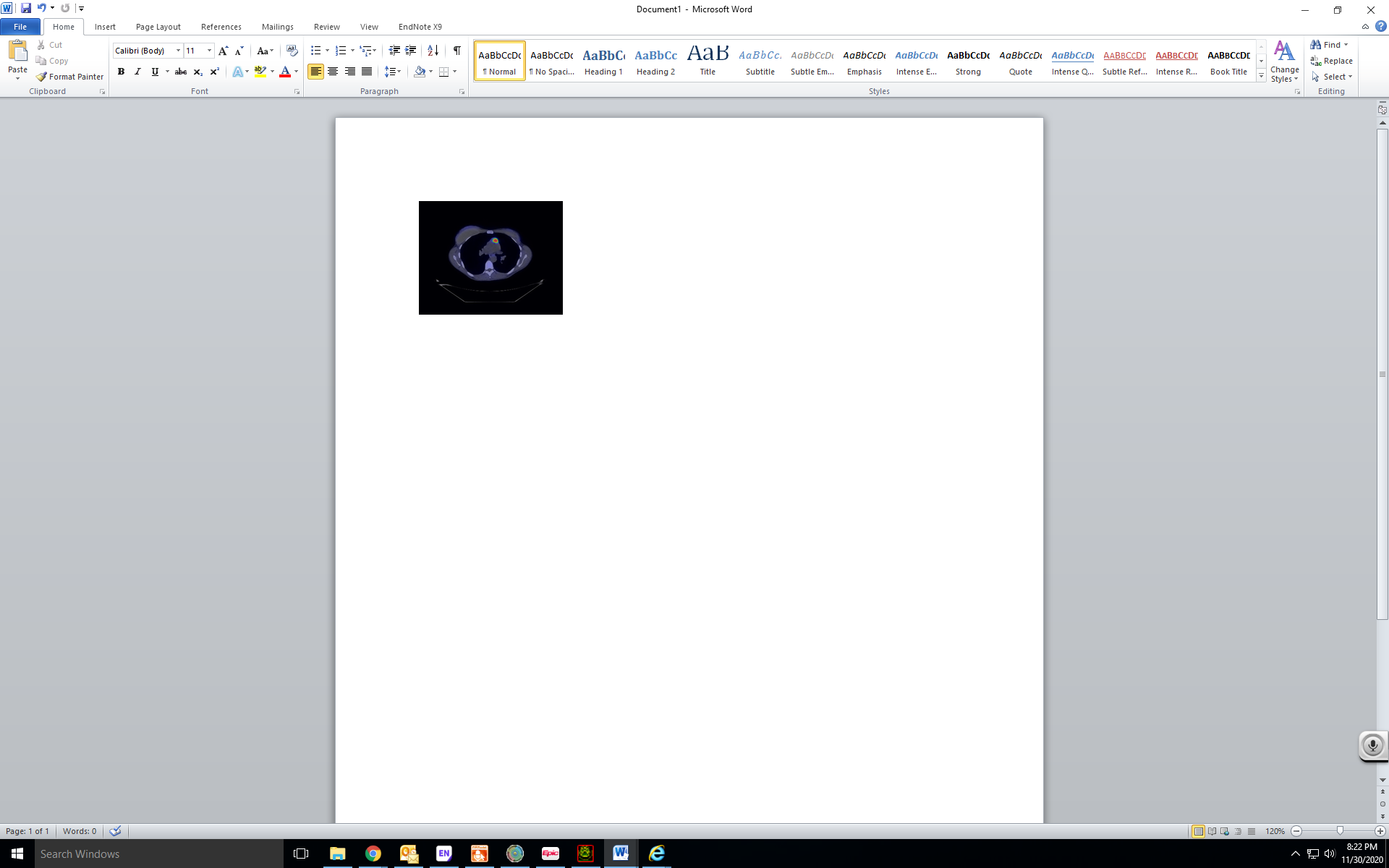
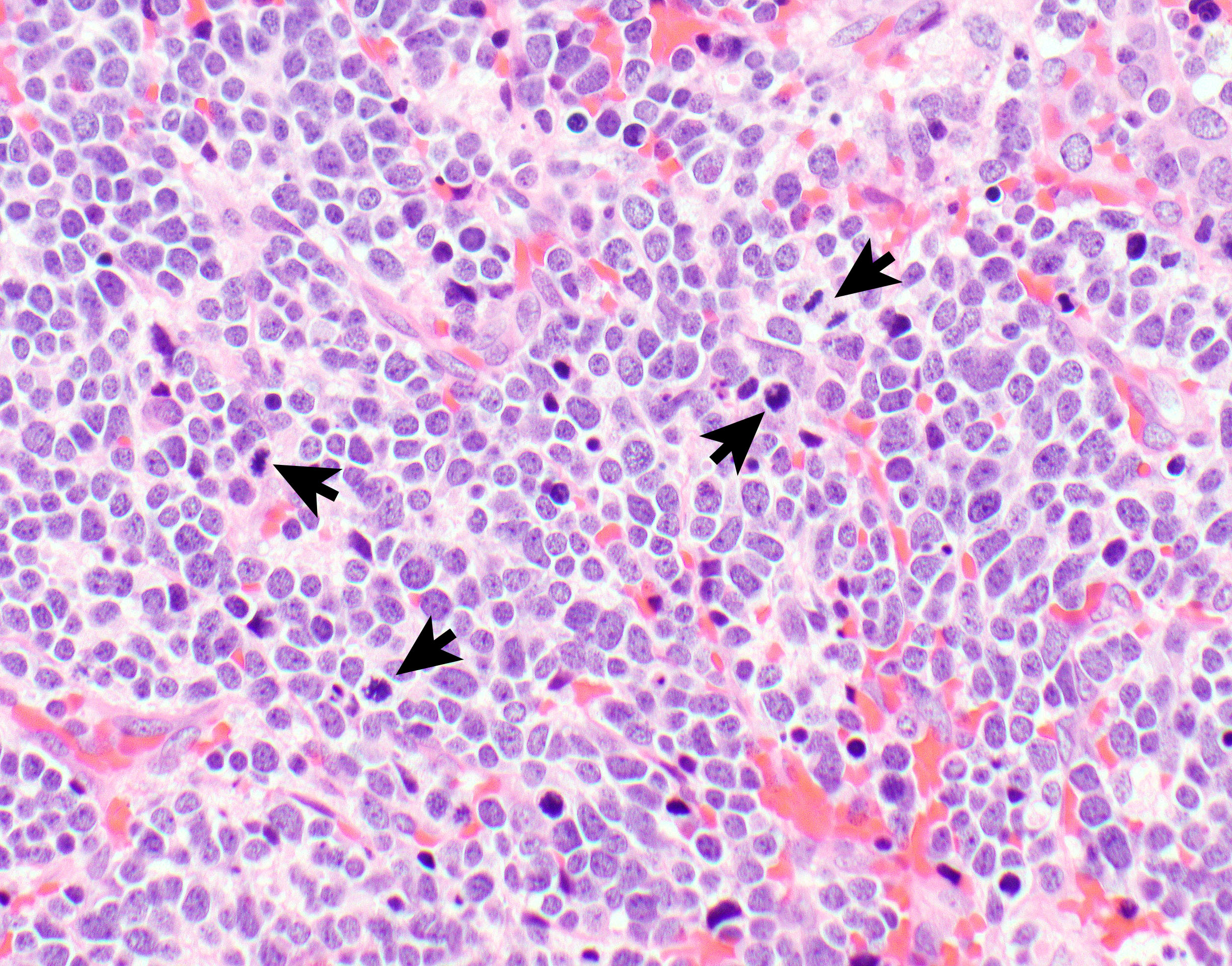
Case Presentation: A 41-year old female was hospitalized for management of SIADH causing refractory hyponatremia. Her medical history was notable for generalized anxiety disorder and cosmetic silicone bilateral breast implant. She was up to date on age appropriate cancer screening, and was not taking any prescription medications or supplements. The patient had been in usual state of health until approximately 2 months before this presentation, when she started experiencing frequent episodes of nausea and vomiting. On initial evaluation, her sodium was 110, serum osmolality (SOsm) 232, urine osmolality (UOsm) 200 and random urine sodium (Una) 67. Other labs including ACTH, cortisol, TSH levels, and paraneoplastic antibody panels were unremarkable. Magnetic Resonance Imaging (MRI)brain, Computed Tomography (CT) chest/abdomen/pelvis were all unrevealing. Her hyponatremia was attributed to Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). She was hospitalized and received hypertonic saline with transient improvement in sodium to 127. After 3 days, she was discharged on salt tablets, fluid restriction and oral furosemide. Due to persistent symptoms, she was admitted again with laboratory values remarkable for SNa 120, SOsm 249, UOsm 875 and random UNa 240. Further work up with Positron Emission Tomography (PET) CT demonstrated intra-thymic 2.4 cm x 1.7 cm anterior mediastinal mass with avid DOTATATE uptake (figure 1). She underwent thymectomy with histopathology confirming small cell carcinoma of thymus (figure 2). There were no post-operative complications. Repeat PET CT after procedure did not show evidence of disease. SNa levels (144 mEq/L), SOsm, UOsm completely normalized next day of the procedure. Subsequently, she was evaluated by oncology and cancer-directed chemo radiation therapy was instituted.
Discussion: SIADH is the most common cause of hyponatremia in euvolemic hospitalized patients. It is also the most frequent cause of hyponatremia in cancer patients [1]. Hyponatremia is associated with high morbidity and mortality and causes significant cost burden to healthcare system. SIADH can be due to variety of causes including central nervous system disorders, medications, infections (e.g. HIV), surgery, pulmonary disease, malignancy or idiopathic [2]. It should be suspected in hyponatremia patients appearing clinically euvolemic with SOsm 100 mOsm/kg, urine sodium >20 mmol/L, in the absence of diuretic use, thyroid or adrenal abnormalities. Accurate and timely diagnosis is essential for appropriate management of SIADH. Our patient’s laboratory findings were consistent with SIADH. Given refractory hyponatremia and unrevealing work up, PET CT helped establish cause of SIADH. Generally, thymomas represent malignancy, immunologic or endocrine disorders. About 30-50% thymomas manifest as myasthenia gravis [3]. Our case is one of the few cases reported in literature describing antidiuretic hormone secreting thymic mass.
Conclusions: This case highlights the importance of recognizing one of the rarest causes of refractory hyponatremia as prompt work up and subsequent management can hugely affect outcomes.