Background: Catheter-associated urinary tract infections (CAUTIs) are associated with increased mortality and length of stay and are a quality metric and focus of quality improvement efforts in many health systems. The degree to which CAUTIs are preventable, however, remains unclear, as some patients require an indwelling urinary catheter (IUC).
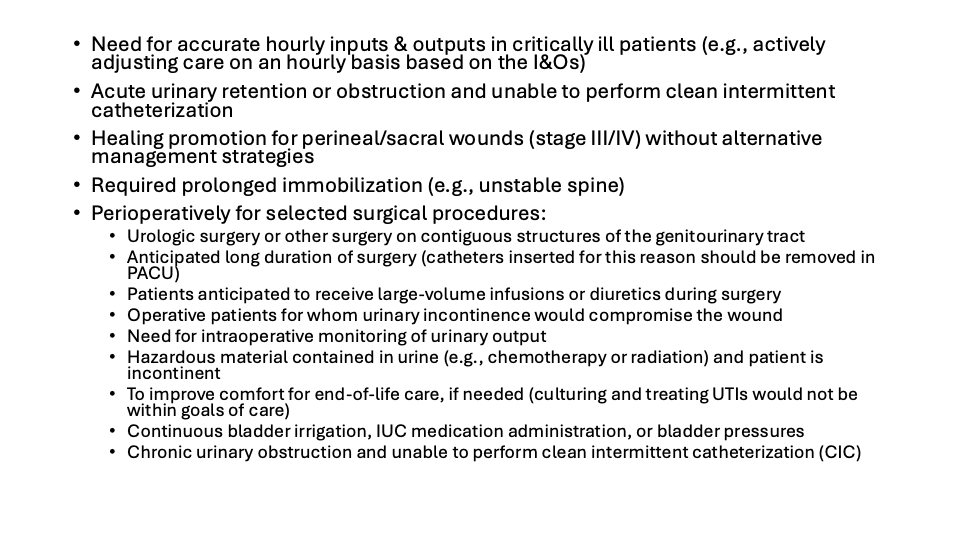
Methods: This was a retrospective study of adult hospitalized patients at an academic tertiary care center. Every CAUTI incident, as deemed by Hospital Epidemiology and Infection Prevention (HEIP) based on the Centers for Disease Control and Prevention’s National Healthcare Safety Network (NHSN), prompts a multidisciplinary CAUTI huddle, during which stakeholders from hospital medicine (including the attending at the time of the CAUTI), bedside nursing, nursing leadership, and HEIP. This huddle entails proceeding through a standardized checklist that identifies missed opportunities for infection prevention, including via evaluating the appropriateness of the IUC and bedside nursing-driven IUC-associated best practices. Using CAUTI huddle data collected between July 2024 and October 2025 and chart review, we determined whether the IUC in place had been for an indication deemed appropriate by our institution’s guidelines (Figure 1), then graded the IUC’s appropriateness as appropriate, not appropriate, and indeterminate, and tallied the specific reason each CAUTI episode warranted such a grade.
Results: In a 15-month period, there were 63 CAUTIs. Thirty-six (57%) were among patients with a true indication for an IUC; 24 (38%) occurred among patients in whom IUC placement was not appropriate; and 3 (5%) were in patients in whom IUC placement was of unclear appropriateness. The most common reasons for the inappropriate presence of IUC among patients with CAUTI were that the clinician/team did not attempt straight catheterization (15/24, 62.5%), the patient declined straight catheterization (3/24, 12.5%), and that the indication for the IUC was intake and output less frequently than hourly (3/24, 12.5%).
Conclusions: Among patients diagnosed with CAUTI based on NHSN criteria, more than one-third had an IUC in place for an indication not considered appropriate based on HEIP criteria at our institution. This indicates further education around indications for Foley placement could have a role in preventing a significant number of CAUTIs. Education for clinicians around straight catheterization rather than IUC placement and the need for IUC placement for Is and Os only if being measured hourly would help prevent CAUTIs by decreasing prevalence of IUC placement. In addition, patient education around straight catheterization and the dangers of IUC placement also would be helpful.