
Background:
The assessment of patients with acute chest pain (CP) remains a continuing clinical problem, with major logistic and financial implications for health care providers. Although appropriateness criteria for stress echocardiography (SE) were unavailable at the time of this study, we applied published stress nuclear appropriateness criteria for CP assessment to SE and studied the trend of use of stress modalities for CP evaluation,
Methods:
All patients presenting to the CP unit between February and March 2007 were reviewed. Patients with any documented coronary disease were excluded. The study group was classified as very low, low, intermediate, or high risk for coronary artery disease by Diamond‐Forrester (DF) criteria. Stress testing was ordered by the CP unit hospitalists. We followed our stress lab protocol of stress nurse/cardiologist determining exercise capacity of patients prior to doing any pharmacologic stress tests. Two board‐certified cardiologists reviewed all rest electrocardiograms for diagnostic interpretability of exercise ischemia and were provided information on the type of test done along with the DF risk stratifications. They scored need for an imaging test as appropriate (A) or inappropriate (I) based on DF criteria and clinical presentation and presenting EKG interpretability for stress‐induced ischemia.
Results:
Of the 200 screened patients, 120 qualified for the study. Mean age was 57 ± 14 years. Men formed 61 % of the study group in a predominantly African American population (81%). SE was the predominant test used in 85% (exercise echo in 57, dobu‐lamine echo in 45), with 14 nuclear stress tests and only 4 treadmill tests. DF criteria were applied to 120 patients with chest pain as their indication for a stress test. The results showed 6.67% were very low probability, 15.83% low probability, 71.67% intermediate probability, and only 5.83% high probability per DF criteria for likelihood of coronary disease. Overall, 75 tests (62.5%) were A and 45 (37.5%) were I, meaning an imaging study was not indicated. Eighteen of 27 patients (66%) in the <10% likelihood by DF criteria had an I test; 93% of the I tests were an exercise echo. Only 1 of 27 tests in the low‐likelihood DF was reported to be abnormal.
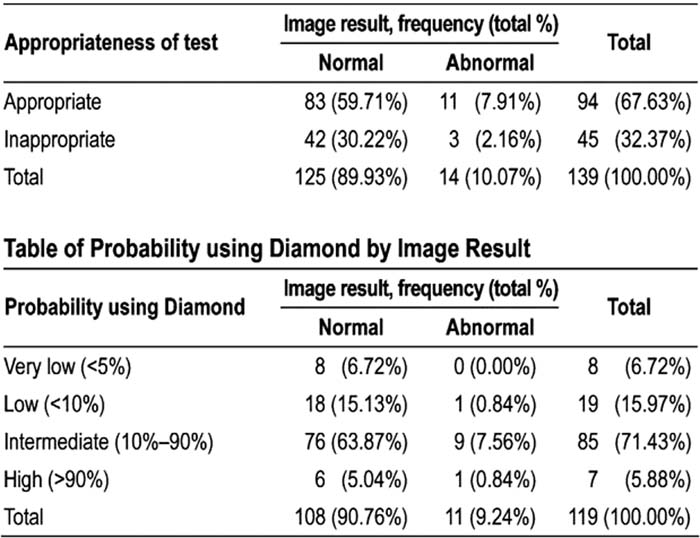
Table of Appropriateness of Test by Image Result
Conclusions:
Routine use of stress imaging tests by CP units poses a significant financial burden on health care systems. Based on our hospital charges of approximately $184 for a treadmill and $507 for a comprehensive stress echo, a cost savings of approximately $14,535 could have been achieved by doing a treadmill test on 45 of patients with an I imaging test. Educating hospitalists and emergency physicians on risk assessment and testing tools for CP and using less expensive treadmill testing for low‐risk patients will result in substantial savings without compromising patient care.
Author Disclosure:
E. Akhras, none; M. Abdul‐Malek, none; N. Salem, none; K. Ananthasubramaniam, none.