Background: We have previously showed how implementing the Michigan Appropriateness Guide for Intravenous Catheters (MAGIC) to inform peripherally inserted central catheter (PICC) use can lead to more appropriate device use. In this analysis, we assessed the association between appropriateness and PICC-related complications. We hypothesized that improved PICC appropriateness is associated with reduced major PICC complications (composite of central line-associated bloodstream infection [CLABSI], venous thromboembolism [VTE], and catheter occlusion).
Methods: We used prospectively collected data from hospitals participating in the Michigan Hospital Medicine Safety (HMS) Consortium to perform this analysis. An evidence-based intervention centered on MAGIC was implemented in HMS hospitals between 2017-2019. Hospitals focused on three appropriateness targets: reducing short term PICC use (< 5 days), increasing use of single lumen devices, and avoiding PICC placement in patients with an eGFR <45 ml/min. Hospitals implemented MAGIC-recommended interventions including clinician education, changes to order-sets, empowering vascular access teams and minimizing use of PICCs in patients with chronic kidney disease. Multi-level mixed effects logistic regression (accounting for patients nested within hospitals) and mixed effects Poisson models (considering rate of events) adjusted for patient-, device- and facility-level covariates were fit to assess the association between MAGIC, PICC appropriateness and complications (composite of CLABSI, VTE and occlusion). Results were expressed as odds ratios (ORs) and interval rate ratios (IRRs) with corresponding 95% confidence intervals (CI).
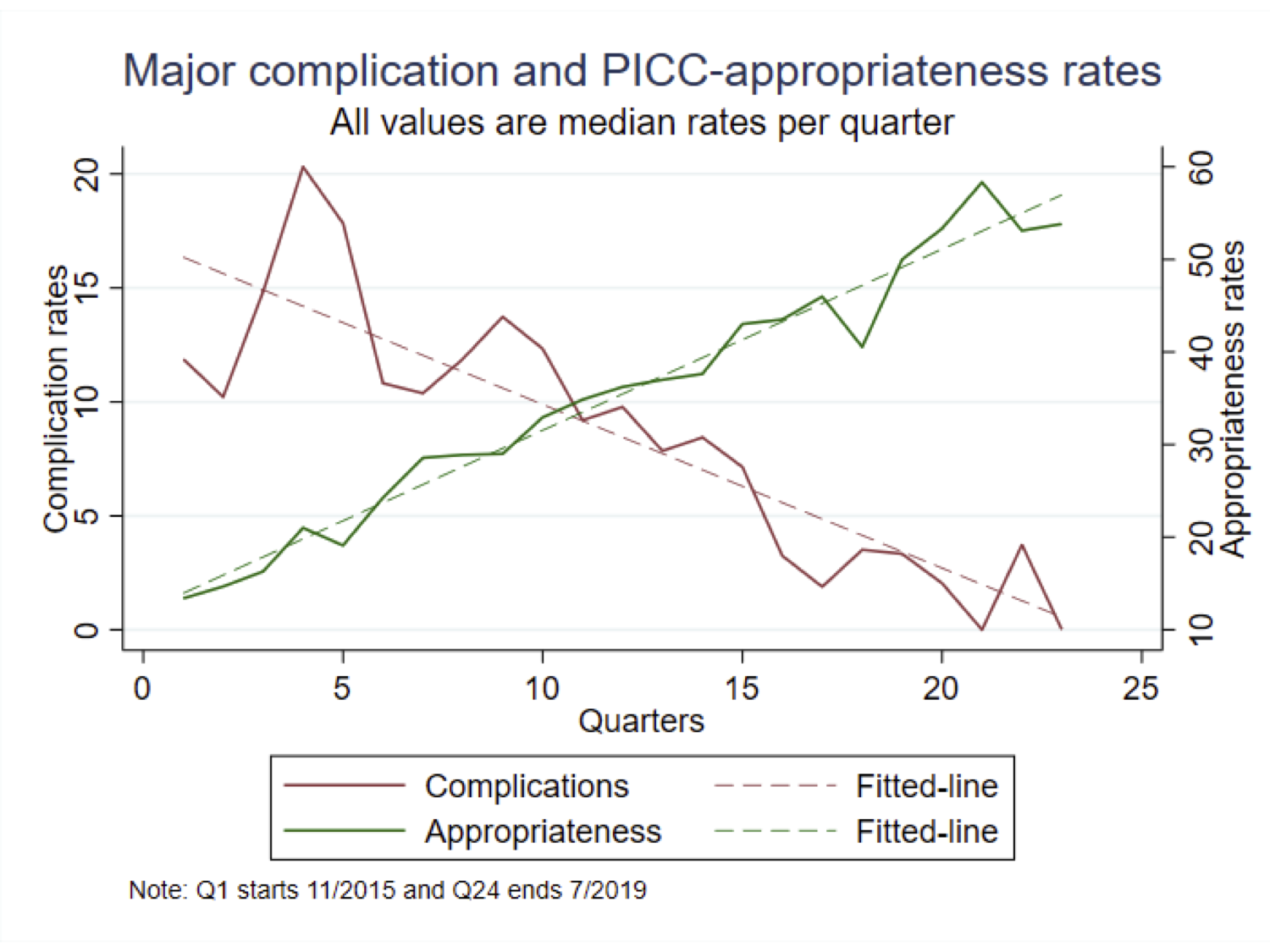
Results: Data from 38,151 PICCs placed in 52 hospitals were available for analysis. Median duration of PICC use at each hospital ranged from 9 to 33 days. The baseline rate of inappropriate PICC use (composite of <5 days, multi-lumen use, and PICC use in patients with eGFR<45) was 31.7%. Similarly, the baseline rate of complications prior to implementing MAGIC was 3.3% for VTE, 1.9% for CLABSI, and 10.6% for catheter occlusion.Following implementation of MAGIC, PICC appropriateness improved from 31.71% to 48.37% (p<0.001) across sites. Compared to patients with inappropriate PICC placement, appropriate PICC use was associated with a 66% reduction in the incidence of major complications (OR 0.34, 95% CI 0.31 - 0.38). Specifically, implementing MAGIC was associated with a reduction in catheter occlusion (OR 0.25, 95%CI 0.22-0.27), CLABSI (OR 0.66, 95%CI 0.53-0.81) and VTE (OR 0.46, 95%CI 0.40-0.61, p<0.001 for all). For every 1% increase in appropriateness at a hospital, major complications declined at a rate of 0.33 [IRR 0.33, 95% CI (0.22 – 0.49). The appropriateness metric that improved the most following MAGIC implementation was single-lumen device use (from 42.2% - 59.7%). Correspondingly, the major complication that declined the most was catheter occlusion (from 10.60% - 7.48%).
Conclusions: In this multi-hospital study, implementation of MAGIC was associated with substantial increases in catheter appropriateness and concurrent decreases in major PICC-related complications. Hospitals seeking to improve PICC appropriateness and device outcomes should consider implementation of MAGIC as a safety strategy.