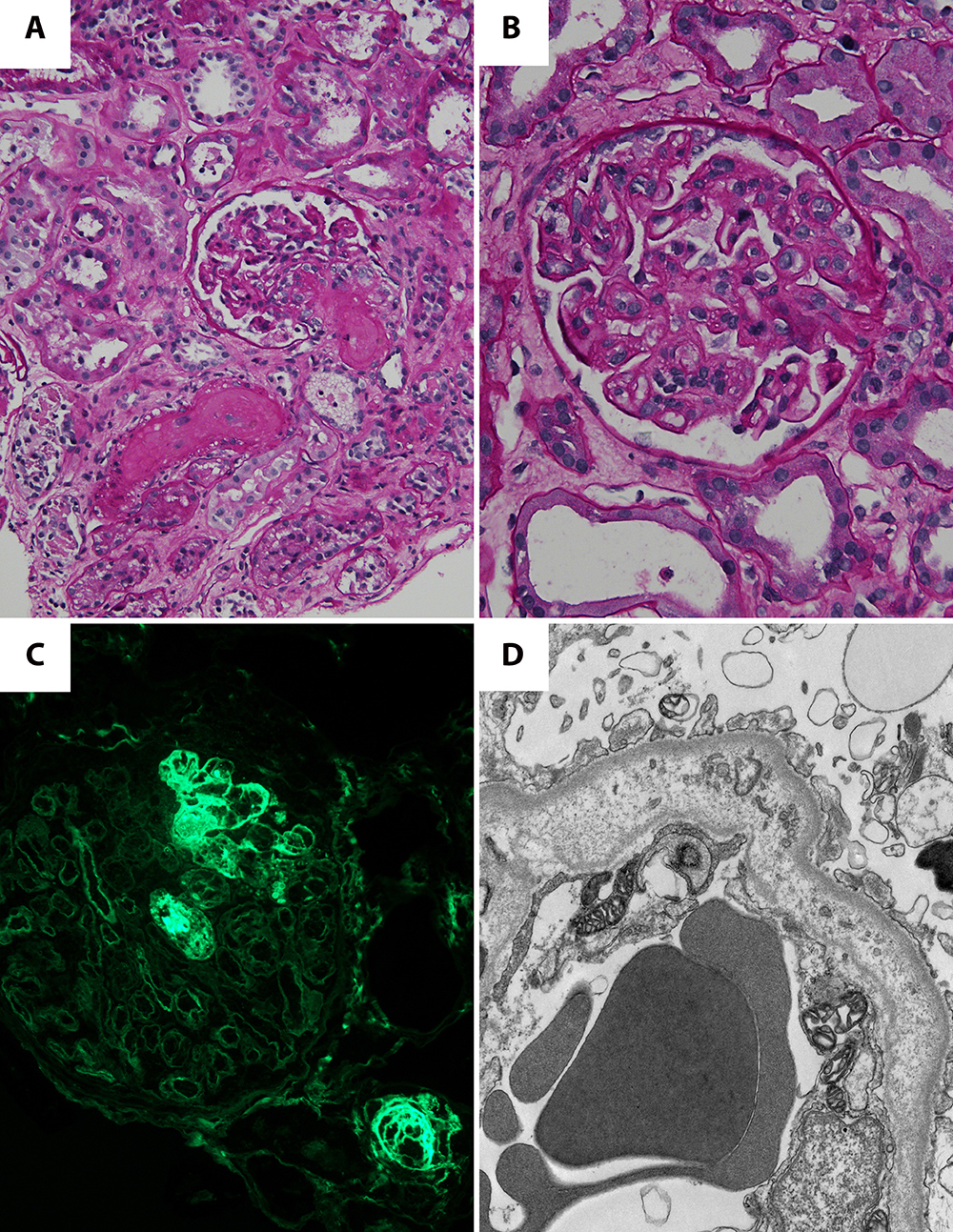
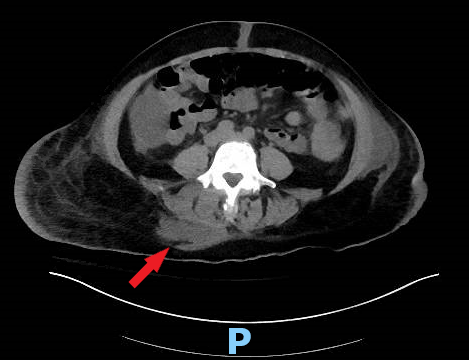
Case Presentation: A 51-year-old woman with irritable bowel syndrome presented with abdominal distention, anasarca, and altered mental status. A few weeks prior to her admission, she received an intragluteal steroid injection at another facility for recently diagnosed sciatica. On admission to outside facility, vital signs were notable for hypertension (BP 171/88). Laboratory work was significant for sodium 111 mmol/L, (nl 135-145 mmol/L), hemoglobin 5 g/dL, (nl 11.5-15.5 g/dL), and creatinine 6.95 mg/dL (nl 0.50-1.3 mg/dL). Blood cultures were positive for MSSA of unclear source. She was admitted to the ICU for uremic encephalopathy requiring emergent hemodialysis via right chest wall permcath and was started on nafcillin for MSSA bacteremia. She was then transferred to our tertiary medical center for further work up and management of her renal failure. Further work up showed LDH 1654 U/L (nl 50-250 U/L ) ADAMTS13 37.3%, platelets 148 K/uL (nl 150-400 K/uL), normal complement levels (C3 and C4), and normal serum quantitative HCG. On hospital day 3, she underwent kidney biopsy which subsequently showed acute thrombotic microangiopathy (TMA) (Fig 1). She was also having diarrhea; stool studies were negative for Shigella and Shiga-toxin producing E. coli. She was immediately started on eculizumab given high suspicion for atypical HUS. CT abdomen/pelvis without IV contrast was done to evaluate for MSSA source was notable for a right gluteal 7.4 x 4.1cm fluid collection that was not observed at the other facility (Fig 2). A drain was placed in the fluid collection by interventional radiology; fluid culture grew MSSA. Genetic testing sent later was positive for atypical HUS. After hemodialysis nearly every day for 10 days, her mental status returned to baseline. On hospital day 28, the patient was discharged home with a six-week course of cefazolin, and she continued to receive dialysis for six weeks.
Discussion: Atypical HUS is a rare disease that has been reported to be associated with bacterial upper respiratory infections, gastroenteritis, or pregnancy (1). More frequently, atypical HUS is associated with diarrhea caused by Shigella or Shiga-toxin producing E. coli in the stool. Our patient initially presented with classic findings of microangiopathic hemolytic anemia including anemia, thrombocytopenia, renal failure, and neurologic changes. ADAMTS13 activity excluded thrombotic thrombocytopenic purpura (TTP). Renal biopsy showed TMA, and genetic testing confirmed the diagnosis of atypical HUS. Stool studies were negative for Shigella and Shiga-toxin producing E. coli. Serum quantitative HCG was normal. The suspected possible trigger was the MSSA bacteremia from the gluteal abscess likely caused by her recent steroid injection. For many years, the treatment of choice for atypical HUS was plasma exchange, which effectively treats patients with anti-factor H antibodies (2). Plasma exchange could induce remission in patients without anti-factor H antibodies, but did not prevent renal deterioration. Eculizumab has demonstrated its efficacy in treating atypical HUS and preventing renal failure (3).
Conclusions: Atypical HUS is a rare disease which is sometimes caused by various types of infections. However, this is the first reported case of S. aureus bacteremia triggering atypical HUS. Atypical HUS should be considered for all patients with thrombotic microangiopathy. Anti-c5 antibodies such as eculizumab not only treat atypical HUS but also prevent renal deterioration.