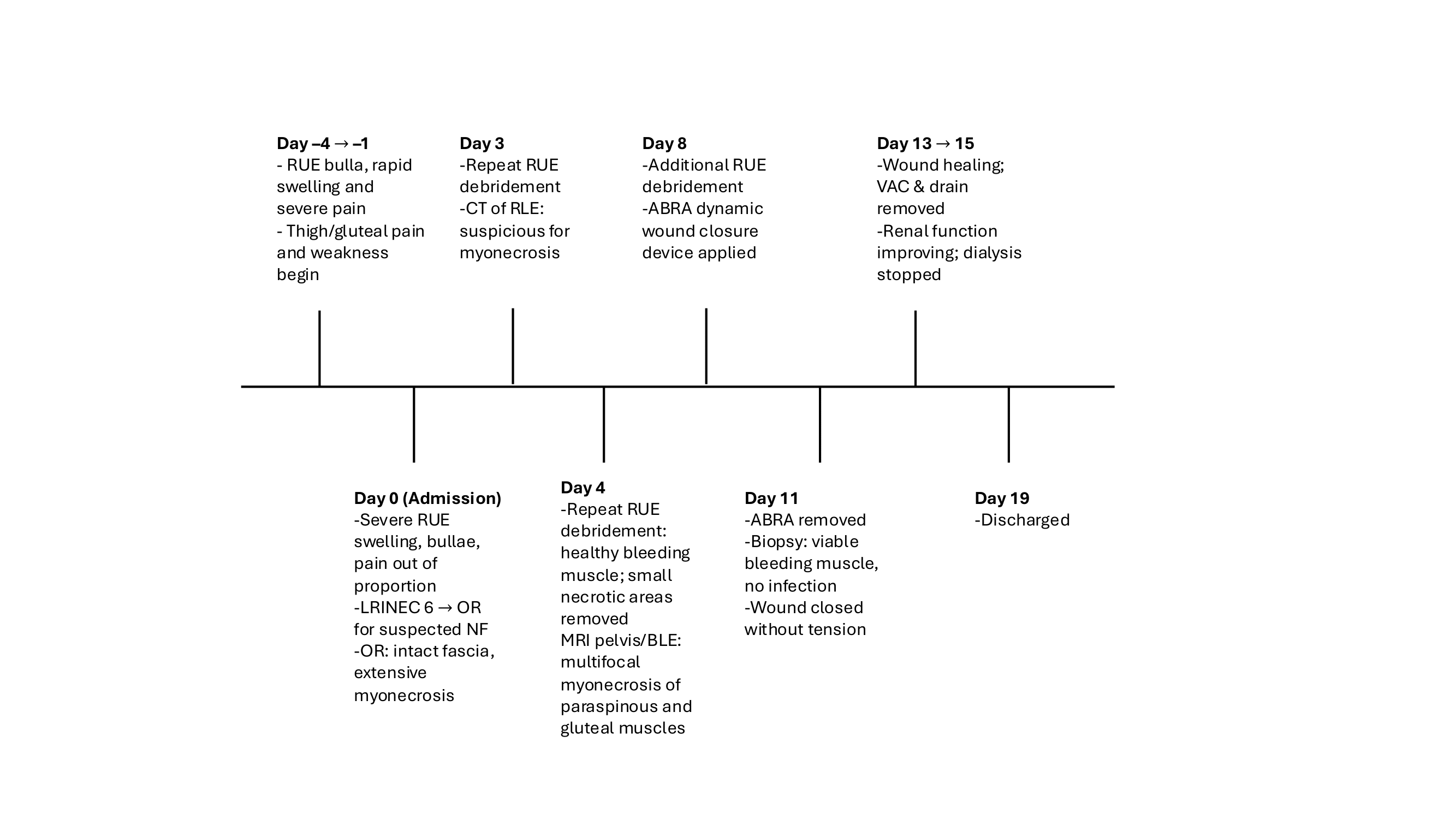
Case Presentation: A 43-year-old man with no significant past medical history presented with 3–4 days of rapidly progressive right upper extremity pain, swelling, and bullae. Symptoms began with a bulla at the antecubital fossa and extended distally and proximally. He also developed bilateral thigh and hip cramping with difficulty walking. He denied trauma or IV drug use, though urine drug screening was positive for cocaine. Labs revealed hyponatremia (Na 124 mmol/L), acute kidney injury (Cr 10.9 mg/dL), metabolic acidosis, CK >39,000 U/L, leukopenia, and elevated inflammatory markers, yielding an LRINEC score of 6.Because of pain out of proportion, rapid progression, and bullae, emergent surgical exploration was performed for suspected necrotizing fasciitis. Intraoperatively, the fascia was intact, but the extensor compartment showed friable, necrotic, non-contractile muscle, requiring debridement of multiple extensor muscles. Imaging later demonstrated multifocal myonecrosis of the quadratus femoris, gluteus medius, vastus intermedius, and paraspinous musculature without fascial involvement. Blood and wound cultures and 16S PCR were negative. Autoimmune myositis testing, including ANCA and extended myositis panel, was unrevealing. His hospital course was complicated by acute tubular necrosis with anuria requiring temporary hemodialysis. He underwent multiple debridements and wound VAC therapy with eventual successful wound closure.
Discussion: This case highlights the diagnostic challenge of distinguishing necrotizing fasciitis from noninfectious myonecrosis, particularly when clinical features overlap. The patient initially met several high-risk criteria for necrotizing soft-tissue infection, including rapid progression, pain out of proportion, bullae, systemic toxicity, and an elevated LRINEC score. However, operative findings, imaging, and histopathology ultimately demonstrated multifocal myonecrosis with preserved fascia, minimal inflammation, and negative cultures.Cocaine and its adulterants, especially levamisole, are increasingly associated with soft-tissue injury, vasculitis, and necrosis. Most reported cases involve cutaneous necrosis or ANCA-positive vasculitis rather than isolated or multifocal myonecrosis. In this case, the absence of ANCA positivity or vasculitic skin lesions, combined with multifocal muscular involvement, suggested a toxic or ischemic mechanism rather than infection. This uncommon presentation expands the spectrum of cocaine-related tissue injury and demonstrates how drug-induced myonecrosis can closely mimic necrotizing fasciitis clinically and histologically.
Conclusions: This case demonstrates that multifocal, noninfectious myonecrosis can mimic necrotizing fasciitis and trigger emergent surgical intervention. Negative cultures, intact fascia, multifocal involvement, and lack of autoimmune markers supported a toxic etiology likely related to cocaine exposure. Clinicians evaluating rapidly progressive soft-tissue injury should maintain a broad differential, integrate multimodal diagnostics, and consider drug-induced myonecrosis when findings are atypical for necrotizing fasciitis.