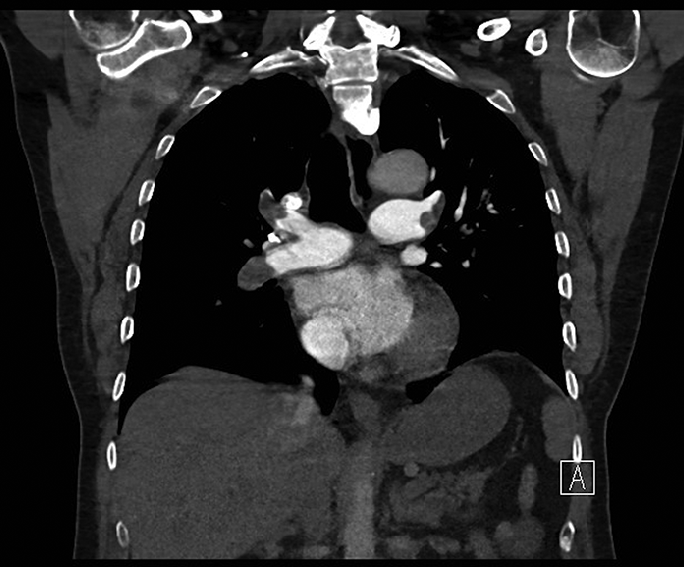
Case Presentation: An 82-year-old female with history of dementia, hypertension, and diabetes, presented with nausea, 2 episodes of nonbilious vomiting, and generalized weakness for 1 day. She was hypotensive (73/52 mmHg) and hypoxic, requiring 4L nasal cannula oxygen to maintain saturations, but without any respiratory distress. Influenza and COVID testing was negative, but chest imaging demonstrated right lower lobe pneumonia. Labs revealed elevated lactate (3.0) without leukocytosis, acute kidney injury (creatinine 2.2 mg/dl), and up-trending troponins with nonischemic EKG. Blood pressure and lactate improved with intravenous fluid resuscitation. Blood cultures were drawn and the patient was started on antibiotics. An echocardiogram revealed global hypokinesis with mildly decreased left ventricular ejection fraction (47%), severe tricuspid regurgitation, and severely elevated pulmonary artery systolic pressure (64 mmHg) with dilated inferior vena cava. CT chest angiogram was obtained and demonstrated large occlusive and nonocclusive pulmonary emboli in bilateral main pulmonary arteries extending into distal lobar and segmental branches with significant right heart strain. CT abdomen with contrast revealed abdominal aortic thrombosis extending into the right renal artery with consequent renal infarction. Bilateral lower extremity non-occlusive deep vein thrombi were also noted. Patient was started on heparin infusion and hypercoagulability workup was initiated. While anti-beta-2-glycoprotein and anticardiolipin antibodies were negative, lupus anticoagulant was positive, confirming the diagnosis of CAPS in the setting of extensive venous and arterial thrombi. Despite therapeutic anticoagulation and supportive care her renal function worsened with creatinine trending up to 9 mg/dl and the patient becoming oliguric. At this point, the family opted to forgo aggressive interventions including plasma exchange and dialysis. Patient was discharged to home hospice on steroids to mitigate further thrombotic events.
Discussion: An acute CAPS episode is often triggered by an infection as seen in our patient. Pathogenesis involves APS antibody mediated complement and coagulation cascade activation resulting in accelerated diffuse thrombosis. Incidence is usually in relatively young women in their 40s unlike our octogenarian patient. Data from CAPS Registry show that the most commonly involved organs are the kidneys (74%), brain (56%), lungs (55%), and heart (53%). Thrombotic microangiopathy with thrombocytopenia and microangiopathic hemolytic anemia with schistocytes are seen on peripheral smear.
Conclusions: CAPS is managed with systemic anticoagulation in the absence of major bleeding, in addition to glucocorticoids, therapeutic plasma exchange, and/or intravenous immunoglobulin. Rituximab and eculizumab may also be used.