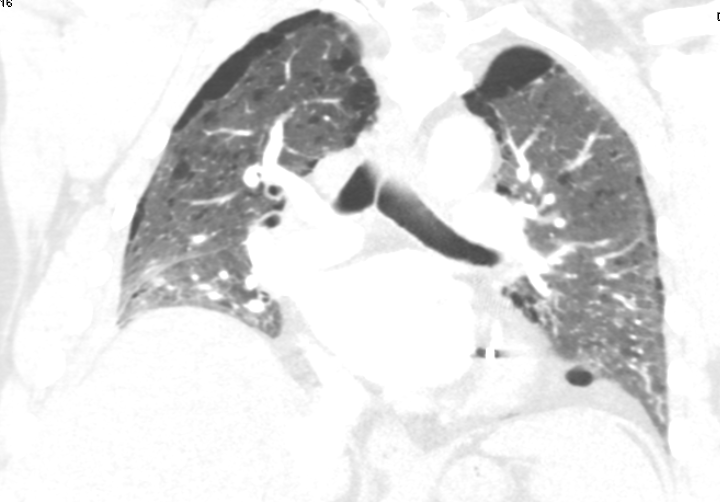
Case Presentation: A 73-year old male, retired autoplant machine technician presented to the ED two weeks ago for a three-day history of progressively worsening shortness of breath likely secondary to a COVID-19 positive infection. His past medical history included Stage IV adenosquamous carcinoma of the right lung status post chemotherapy, provoked pulmonary embolus on anticoagulation, interstitial lung disease, Chronic Obstructive Pulmonary Disease (COPD) on two liters nasal cannula at baseline, bullous emphysema, former smoker (50-pack year history), and multiple hospital admissions for COPD exacerbations and pneumonia. His medications included arformoterol, ipratropium, levalbuterol, azithromycin, prednisone, benazepril, and apixaban. He took a at home COVID-19 test twice with positive results; he thus arrived at the ED to get further evaluated. He was hemodynamically stable, afebrile, and oxygen saturations were within normal limits on two liters. Another confirmatory COVID-19 test was positive. Two years ago, a Computer Tomography (CT) scan revealed a sizeable bulla measuring 10.6×5.2 cm transversely and 14.2 cm in height, situated in the right lower lobe. Remarkably however the CT Angiography scan to rule out a pulmonary embolus at his ED visit incidentally noted complete resolution of the bulla. The patient was prescribed a course of Paxlovid, and discharged home in a stable state.Astoundingly, during the patient’s pulmonology clinic visit two weeks later, he mentioned a decreased necessity of morphine to treat his air hunger he struggled with for the last couple years. Other than an unspecified episode of greater than usual pain in the right lower chest, the generalized improvement in symptomatology baffled the pulmonology department.
Discussion: Spontaneous emphysematous bullae regression has yet to have a rationale behind the rare occurrence; however, the etiology has been theorized. One school of thought is that resolution occurs up to three weeks after air-fluid level development within a bulla due to peri-emphysematous lung infection. A link between inflammation, connective tissue deposition, and emphysema shrinkage has previously been stated. Although cases with regression of dominant bulla have also been described in association to lung cancer with reasoning yet to be determined. What is shared between literature is that autobullectomy may improve pulmonary functioning. The patient presented in this case may have had resolution of bulla as a consequence of his recent COVID-19 infection. Inflammation-induced connective tissue deposition in the lung parenchyma possibly resulting in the shrinkage of emphysematous lesions. However, his remote history of unspecified right-sided chest pain along with improvement in clinical symptomatology may support the notion of a spontaneous pneumothorax that never received treatment leading to auto pleurodesis.
Conclusions: Emphysematous bullae regression, characterized by the reduction in size and volume of large air-filled spaces within the lungs, represents a captivating phenomenon in pulmonary medicine. This case above highlights the spontaneous regression of a large bulla found incidentally after an active COVID-19 infection, challenging the conventional understanding of this rare occurrence. While the patient symptomatology and over clinical status improved, the rationality behind autobullectomy still remains uncertain.
.png)