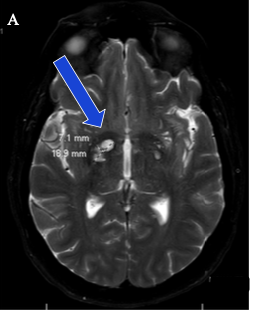
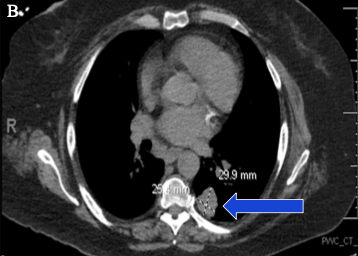
Case Presentation: A 59-year-old immunocompetent woman presented with a one-month history of persistent migraine headaches and two weeks of nausea and vomiting. Initial laboratory workup and CT imaging of the head and abdomen were unremarkable. During hospitalization, she experienced a syncopal episode with seizure-like activity. MRI of the brain revealed hyperintense periventricular and subcortical white matter lesions. Lumbar puncture showed markedly elevated intracranial pressure, low glucose, elevated protein, and a serum cryptococcal antigen titer of 1:2560. CSF culture confirmed Cryptococcus gattii. She was started on liposomal amphotericin B and flucytosine. Follow-up imaging showed evolving cryptococcomas. CT of the chest later revealed a lung mass, with biopsy confirming cryptococcal infection. Due to persistent elevated intracranial pressure and worsening headaches, she required multiple lumbar punctures and ultimately ventriculoperitoneal shunt placement. She completed induction therapy and was discharged on long-term fluconazole.
Discussion: Cryptococcus gattii infection is rare in immunocompetent individuals and often presents with nonspecific constitutional and neurologic symptoms that can delay diagnosis. Early imaging may be normal, and CT scans can miss CNS involvement in up to 50% of cases, underscoring the need for clinical suspicion. Management typically requires prolonged antifungal therapy and close monitoring, particularly when CNS involvement leads to elevated intracranial pressure. Neurosurgical intervention, such as VP shunting, may be necessary. This case highlights the diagnostic and therapeutic complexity of C. gattii infection and the importance of multidisciplinary care.
Conclusions: C. gattii infection in immunocompetent patients is uncommon and may present with subtle yet progressive neurologic symptoms. Early recognition, aggressive antifungal therapy, and management of intracranial pressure are essential to prevent irreversible complications. This case emphasizes the need for heightened awareness when evaluating patients with persistent headaches and atypical CNS findings.