Background: Transitioning from inpatient to outpatient care is high-risk, often associated with harm from incomplete or ineffective communication of clinical information [1]. In one report, 41% of patients had at least one pending study at the time of discharge, 43% of which were abnormal and 9.4% potentially actionable [2]. The discharge summary is a ubiquitous tool used by inpatient providers to communicate clinical information to other clinicians. However, only between 12% and 46% of pending tests are reported on discharge summaries [3]. We sought to incorporate a pending labs “smart list” into a new standardized discharge summary template to assess its effectiveness in communicating pending lab studies in the post-acute care transition.
Methods: This quality improvement initiative employed a pre-post intervention design, set at a large urban academic medical center. We developed a “smart link” in EpicCare electronic health record (EHR) system that compiles a list of pending labs and pathology reports. The pending labs “smart list” was placed into a re-structured discharge summary template defaulted for internal medicine resident and hospitalist physician EHR environments on Jan 18th, 2024 [Fig. 1]. Discharge encounters for general medicine patients were randomly selected for review in a 2-month pre-period, August 1 to September 31, 2023, and a 2-month post-period, January 19 and March 14, 2024. Chart reviews were conducted by 9 resident and hospitalist physician reviewers, with a secondary review by the primary investigator, KN. Our primary measure was the proportion of discharge summaries mentioning all pending labs. Our secondary measures were the proportion of discharge encounters with any pending labs, proportion of discharge encounters with pending labs that resulted abnormal, and proportion of discharges with follow-up notes mentioning post-discharge results. Categorical variables and proportions were analyzed using the Chi-squared test. This study was formally determined to be quality improvement, not human subjects research, and was therefore not overseen by the Institutional Review Board, per institutional policy.
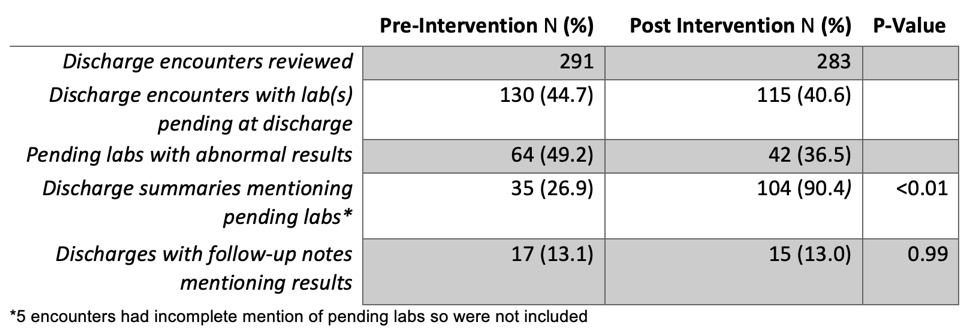
Results: We reviewed 299 of 1561 pre-intervention and 294 of 1410 post-intervention discharge encounters via random selection. 8 pre and 11 post-intervention encounters were excluded due to duplication, death during the encounter, and employee encounters. There were 130 (44.7%) and 115 (40.6%) encounters with 1 or more labs pending at discharge in the pre and post-intervention groups, respectively. Of the encounters with pending labs, 49.2% pre-intervention and 36.5% post-intervention had abnormal results. 35 (26.9%) discharge summaries listed all pending labs in the pre-intervention group compared to 104 (90.4%) in the post-intervention group, p-value < 0.01, [Table 1]. The proportion of discharges with follow-up notes mentioning results post-discharge was not significantly different (13.1% vs 13%, p = 0.99).
Conclusions: Integrating an automated “smart list” that populates pending lab results into the discharge summary template can reliably display pending labs in discharge summaries. However, whether this translated to patients receiving the post-discharge results is unclear. Additional interventions may be required to ensure delivery of discharge summaries, test follow-up, and documentation of reporting results, such as implementing automated discharge summary delivery to primary care providers with confirmatory receipts.