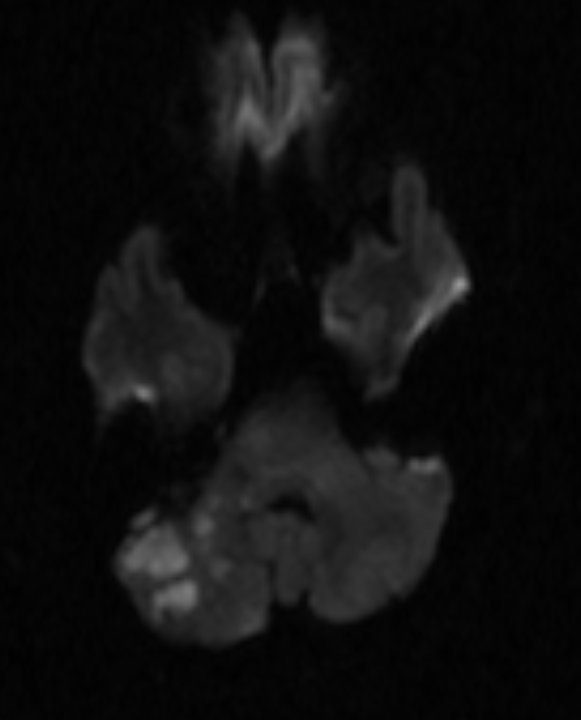
Case Presentation: 57 year old male with history of hypertension, hyperlipidemia, poliomyelitis with right leg atrophy and chronic crutch use presented with right-sided hearing loss, vertigo, and arm numbness. MRI brain and MRA head and neck revealed acute infarction in the right inferior cerebellum in the Anterior and Posterior Inferior Cerebellar Artery territories; left cerebellar chronic lacunar infarct; no flow-limiting stenosis.Further stroke workup included transthoracic echo with bubble, transesophageal echo, hypercoagulable workup, and CT of chest, abdomen and pelvis, all unremarkable. Telemetry was without atrial fibrillation. Hospital day 3 patient reported right arm and hand numbness and coolness. These symptoms started concurrently with the stroke but spontaneously improved so were not reported until symptoms suddenly worsened. Right upper extremity CTA showed occlusive thrombus in the axillary artery and proximal brachial artery. Patient was started on heparin drip and taken for urgent right arm embolectomy. Intraoperative ultrasound showed axillary artery aneurysm with intramural thrombus. Patient subsequently underwent embolectomy, resection of the axillary aneurysm and bypass with saphenous vein graft. Postoperatively patient had return of neurovascular function and was discharged on aspirin and clopidogrel. At six months follow-up he showed complete recovery with no further episodes of stroke.
Discussion: Stroke is a leading cause of hospital admissions [1]. The most common cause of stroke is atherosclerosis followed by cardioembolism. Even after thorough evaluation, around 30% of strokes are cryptogenic [2]. Most cryptogenic strokes are considered embolic strokes of undetermined source (ESUS), especially if the pattern suggests an embolic cause [3]. However studies show anticoagulation is not superior to aspirin in preventing recurrent strokes in patients with ESUS [4], so current secondary prevention for these patients is antiplatelet therapy and vascular risk factor modification [5].Our patient presented with acute cerebellar stroke symptoms, such as vertigo, ataxia, and hearing loss [6]. Concurrently, he experienced intermittent right arm numbness, weakness associated with hand coolness and decreased pulse. The temporal correlation of stroke symptoms with symptoms of arterial occlusion suggests the patient had embolic events from a common source causing both right arm ischemia and right cerebellar infarction. The source of emboli was an axillary artery aneurysm with intramural thrombus. Repeated blunt trauma to the axillary artery results in artery wall weakening and aneurysms [7]. Aneurysms from crutch-use are more frequently complicated by intraluminal thrombus due to sluggish blood flow [8]. The thrombus may dislodge and cause acute, chronic, or repetitive emboli, especially to the affected upper extremity [9]. Very few cases of cerebral embolism from a peripheral arterial occlusion have been reported, and none in the setting of axillary artery aneurysm. The likely mechanism of our patient’s presentation is total thrombosis and lack of forward flow in the axillary artery causing retrograde flow and embolization of the cerebellar artery [10-11].
Conclusions: Axillary artery aneurysm should be considered in patients with risk factors presenting with neurologic or embolic symptoms. It most commonly affects the upper extremity but can be a source of embolic strokes and should be considered in certain patients presenting with cryptogenic strokes.