Case Presentation: A 7-month-old former term female with congenital hypothyroidism was admitted for the third time with a diagnosis of bronchiolitis. Her first admission at 7 weeks of age involved an ICU stay requiring intubation and chest tube placement after a chest X-ray showed a right tension pneumothorax. She suffered no other major complications and was discharged home with supportive care within one week. She presented at 5 months of age with respiratory distress, but had a short hospital stay, and was again discharged with supportive care. On her third admission, she presented with increased work of breathing, but over the course of five days there was no improvement on Vapotherm at 8 L/min, until she was transferred to the ICU and intubated. Pulmonary team was consulted and an echocardiogram (ECHO) was obtained and was normal, however the left pulmonary artery (LPA) was poorly visualized. Bronchoscopy revealed a blind pouch of the right mainstem bronchus and severe bronchomalacia. A chest CT with contrast showed an LPA sling causing moderate narrowing of the distal trachea and proximal right mainstem bronchus. Cardiovascular Surgery then performed LPA sling repair. She tolerated the procedure well; however, she developed a fever post-op. Respiratory culture was positive for Moraxella and a 7-day course of Unasyn was given. She was discharged home on post-op day nine at which point she was tolerating oral feeds and stable on room air.
Discussion: An LPA sling is a rare congenital anomaly in which the LPA arises from the right pulmonary artery and tracks between the trachea and the esophagus to the left lung. Most children present in the first year of life with respiratory symptoms including wheezing, stridor, and recurrent lower respiratory tract infections. An ECHO usually establishes the diagnosis and is also helpful as up to 85% of patients have additional cardiac anomalies. Bronchoscopy can identify tracheal stenosis as this requires surgical repair but is less useful as it does not show the anatomy needed for surgical correction. In contrast, cardiovascular CT angiograms aid in surgical planning. Corrective surgery is the mainstay of treatment for symptomatic patients as without surgery, mortality rate can be as high as 90%. Prognosis is excellent but depends on whether tracheal repair is also required.
Conclusions: Due to nonspecific respiratory symptoms, LPA slings can go unrecognized. As such, it is important to keep a broad differential diagnosis for respiratory distress in pediatric patients. Early identification of LPA slings and repair can lead to improved clinical outcomes.
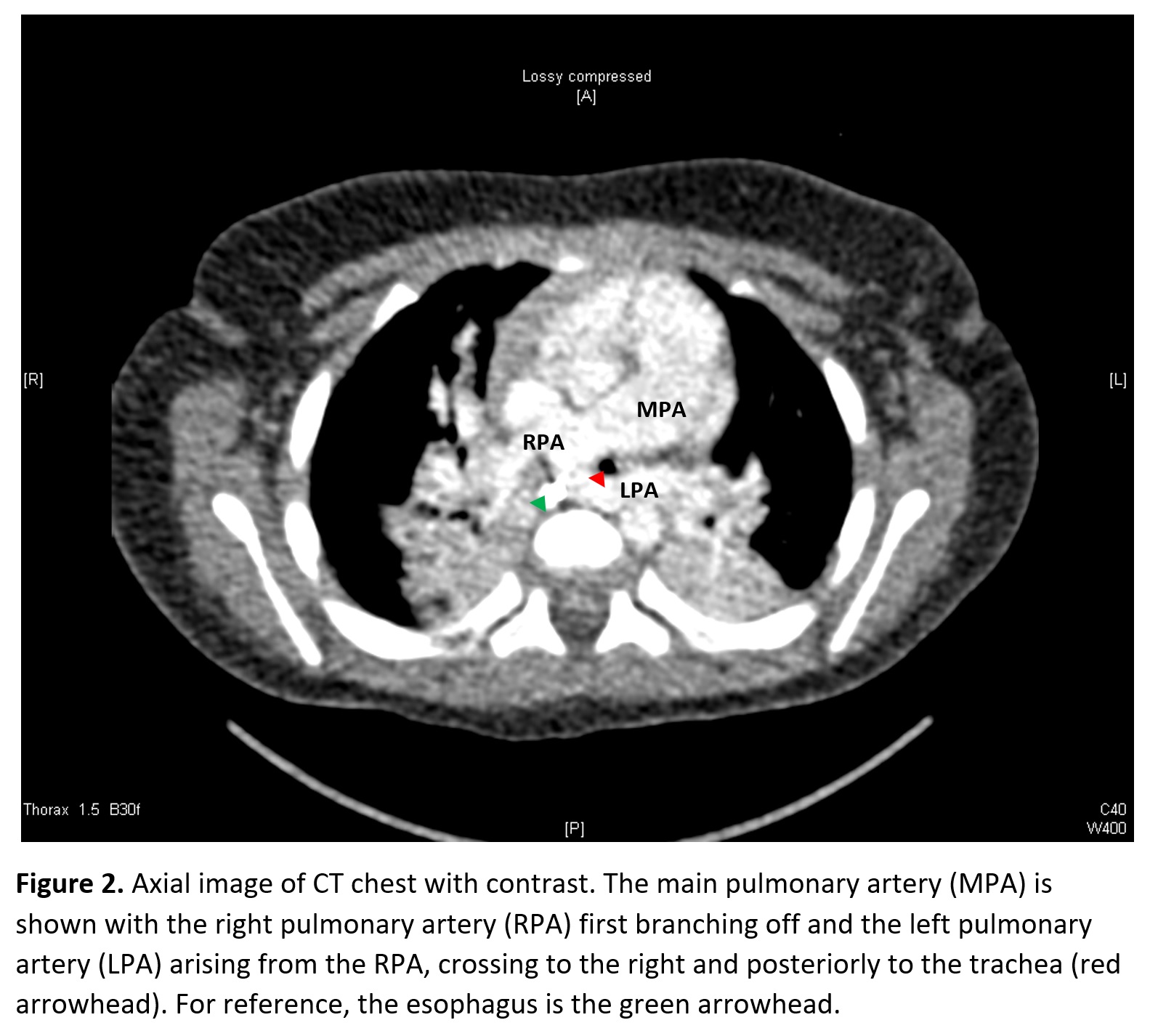
.jpg)