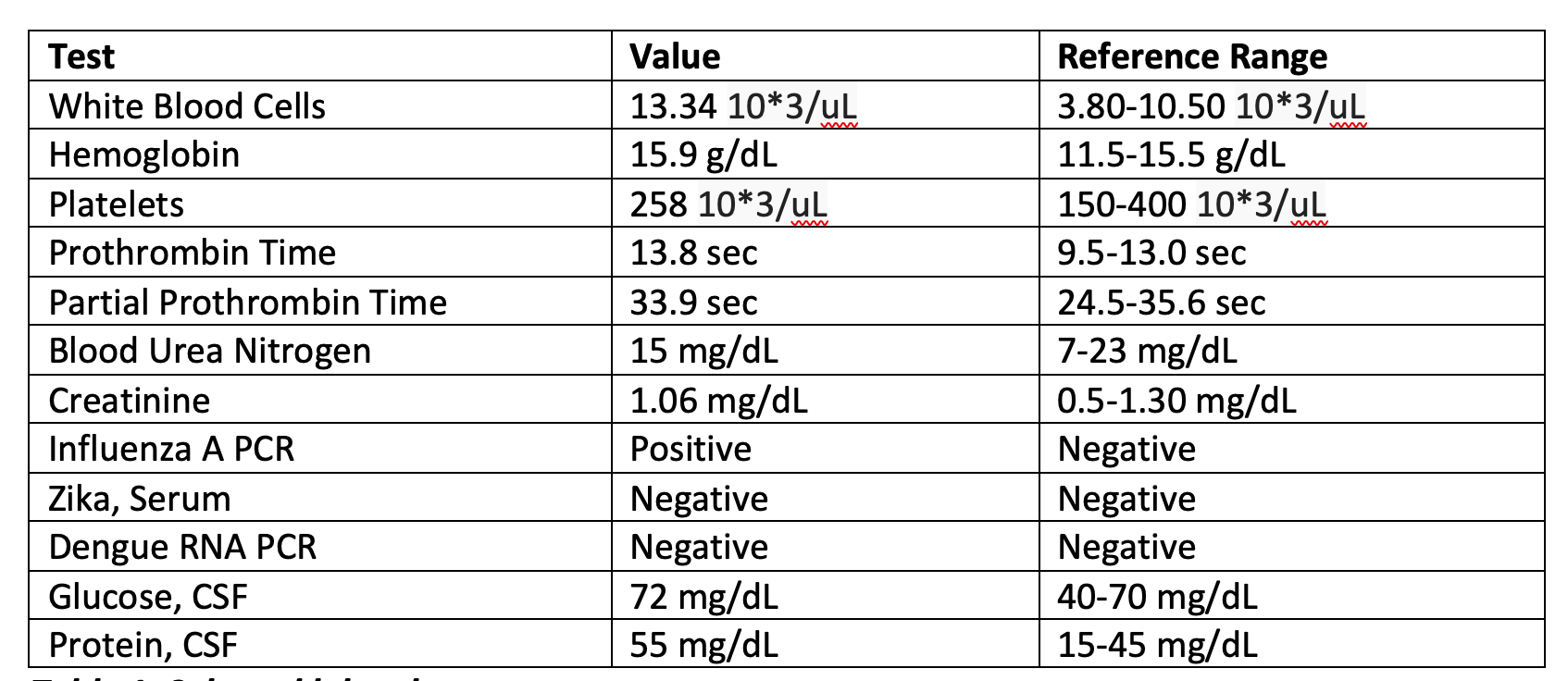
Case Presentation: A 43-year-old previously healthy male presented with acute onset mixed aphasia five days after recovering from an influenza A infection. He was last known well during a normal conversation with family before being found confused and unable to follow instructions at home. In the ED, initial CT and MRI brain imaging showed no acute ischemia, hemorrhage, midline shift, or herniation. Laboratory studies were notable for leukocytosis (WBC 13.34 × 10⁹/L), and urine drug screen was negative. On exam, he was alert and cooperative but exhibited severely impaired comprehension, repetition, naming, and reading, with preserved fluency. Lumbar puncture revealed an opening pressure with WBC 45 cells/µL (80% lymphocytes) and protein 68 mg/dL. CSF PCR was negative for HSV and VZV but positive for influenza A RNA, confirming the diagnosis of influenza-associated encephalitis. Additionally, his course was complicated by seizures in the right temporal lobe. He was treated with IV Peramivir, empiric acyclovir, and supportive care, then transitioned to oral Oseltamivir for a 10-day course. His symptoms resolved completely within five days, and follow-up MRI two weeks later showed near-complete resolution of temporal lobe lesions.
Discussion: IAE is a rare but serious complication of influenza infection, with most cases reported in pediatric populations. In adults, the condition is often underdiagnosed due to its nonspecific presentation. Pathogenesis involves both direct viral neuroinvasion and immune-mediated injury, leading to cerebral edema and encephalopathy. Diagnosis requires a high index of suspicion, especially in influenza season, and should include nasopharyngeal and CSF PCR testing, along with neuroimaging to differentiate IAE from other viral encephalitides such as HSV. Our case demonstrated classic findings, including bilateral temporal lobe hyperintensities on MRI and influenza A detection in CSF.Management strategies are largely supportive but should include early initiation of neuraminidase inhibitors, empiric antiviral coverage for alternative causes until ruled out, and intensive monitoring for complications such as seizures or cerebral edema. Prognosis is variable, with reported adult mortality rates between 10% and 30%. Our patient’s complete neurological recovery underscores the benefit of timely diagnosis and prompt antiviral therapy.
Conclusions: This case of influenza A is very rare in presenting with both a seizure and encephalitis. Influenza-associated encephalitis is a rare but potentially life-threatening complication of influenza in adults. Clinicians should consider IAE in any patient presenting with acute encephalopathy during influenza season. Early neuroimaging, CSF analysis, and molecular diagnostics are essential for accurate diagnosis. Prompt antiviral therapy and supportive care can significantly improve patient outcomes, as demonstrated in this case.