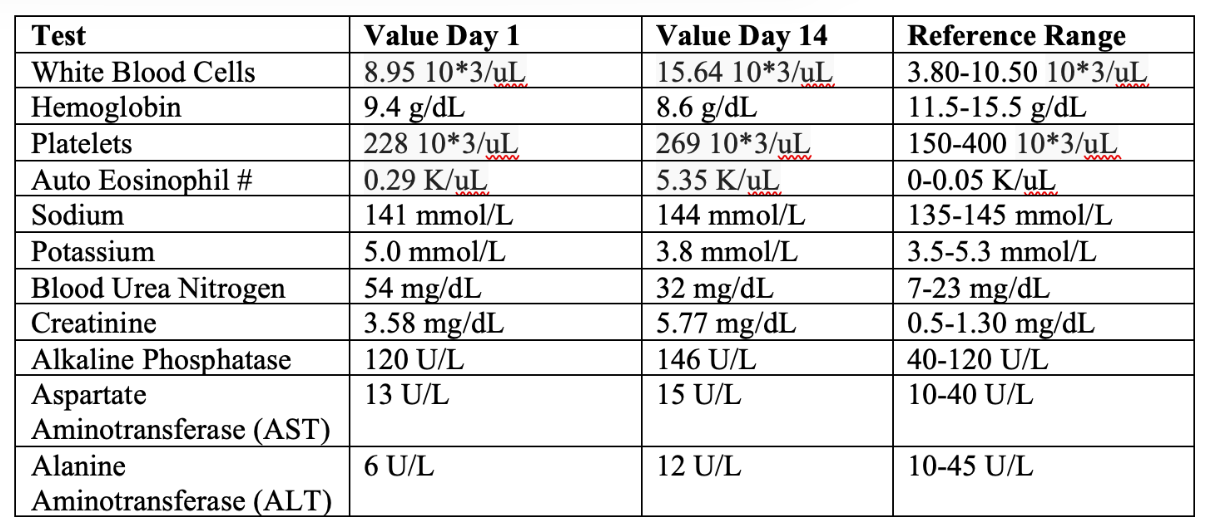
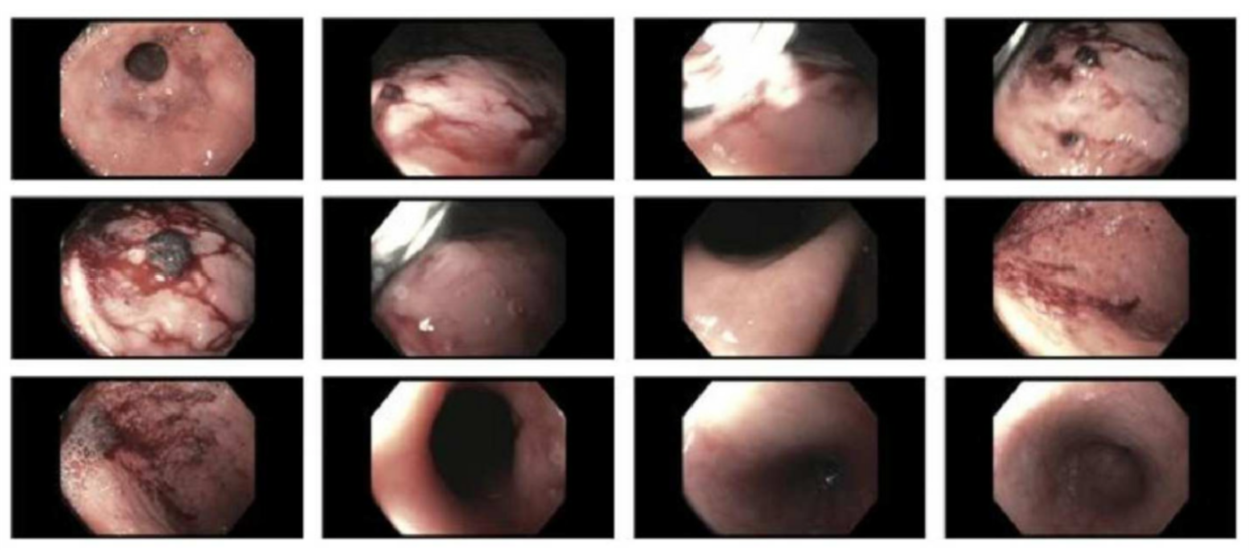
Case Presentation: A 76-year-old woman with end-stage renal disease on hemodialysis, coronary artery disease, and asthma presented with a two-week history of diffuse pruritic rash involving the face and extremities, accompanied by progressive sharp abdominal pain worsened by meals and relieved by defecation. She also reported recent numbness and pain in both toes. Physical examination showed patchy erythematous maculopapular rash, epigastric tenderness, and weak distal pulses. Initial laboratory testing revealed leukocytosis (20.93 K/µL) with marked eosinophilia (4960 cells/µL) and normocytic anemia (10.2 g/dL). Autoimmune, viral, and parasitic etiologies were ruled out. CTA of the chest and aorta demonstrated extensive ulcerated and calcified plaques with mobile embolic components, while vascular imaging showed severe stenoses of multiple arterial beds including bilateral carotids and distal lower extremities, consistent with diffuse atheroembolic disease.The patient received IV methylprednisolone and diphenhydramine, resulting in rapid improvement in abdominal pain and a dramatic drop in eosinophil count to 60 cells/µL, although levels fluctuated between 1050 and 4860 cells/µL throughout her hospitalization. Topical corticosteroids led to mild improvement in rash. On hospital day 10, she developed melena. Endoscopy revealed erosive gastritis and a pre-pyloric ulcer. Her condition declined acutely with abdominal distention, worsening pain, elevated lactate (9.7 mmol/L), and metabolic acidosis. Abdominal X-ray showed colonic dilation. Repeat CT angiography revealed pneumoperitoneum due to perforated bowel. Given her severe baseline comorbidities and poor surgical candidacy, comfort care was initiated, and she passed away shortly after.
Discussion: Eosinophilic gastritis is an rare subset of eosinophilic gastrointestinal disorders characterized by mucosal or transmural eosinophilic infiltration of the stomach without secondary causes such as parasitic infection, drug reaction, or systemic eosinophilic syndromes. Most cases present with nonspecific symptoms, including abdominal pain, nausea, vomiting, and early satiety, often leading to delayed recognition. Gastric perforation is an exceptionally rare complication. In our patient, marked eosinophilic infiltration likely triggered progressive transmural inflammation, weakening the gastric wall and predisposing to perforation. The absence of infectious etiology or vasculitis, combined with peripheral eosinophilia supported the diagnosis. This case underscores the potential severity of EG, particularly when infiltration extends beyond the mucosa to involve deeper layers. Early suspicion is critical, especially in patients with unexplained gastrointestinal symptoms and eosinophilia. Steroids remain the cornerstone of medical therapy; however, acute complications such as perforation may require emergent surgical intervention. The optimal duration of treatment is unclear, and recurrence risk warrants close follow-up.
Conclusions: This case highlights an unusual presentation of eosinophilic gastritis complicated by gastric perforation, emphasizing the need for heightened clinical awareness. Prompt recognition and timely initiation of corticosteroids are essential in preventing severe morbidity. Early multidisciplinary management and long-term monitoring are recommended to reduce recurrence and improve outcomes.