Background: Anti-racism education is increasing across academic institutions; however, physicians have varied levels of skill addressing racist microaggressions. Microresistance Communication Tools (MCTs) are frameworks developed to respond to microaggressions and are common devices used in microaggression trainings. Prior studies evaluating MCT trainings primarily measured change in confidence but rarely objectively assessed ability to apply these skills in clinical or other work settings. It is therefore unclear what impact MCT education has on language or behavior change. Standardized Patient Simulation (SPS) is used frequently in medical education to assess behavioral competency in many domains.
Purpose: Our primary goals were to use SPS methodology to: 1) teach and reflect on microresistance skill acquisition and 2) assess application of skills in a simulated microaggression event.
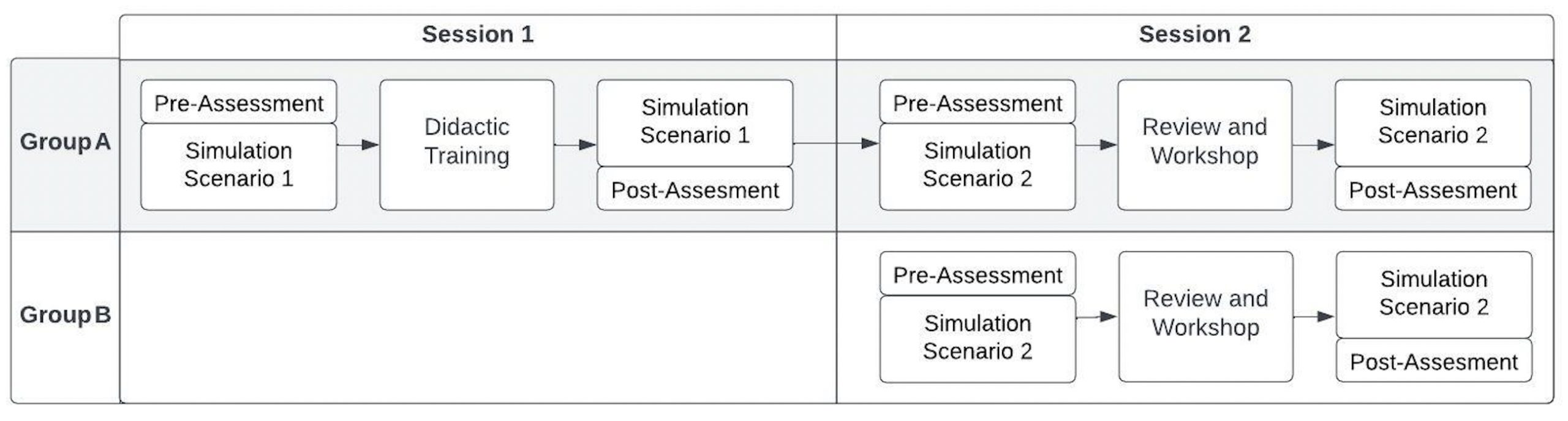
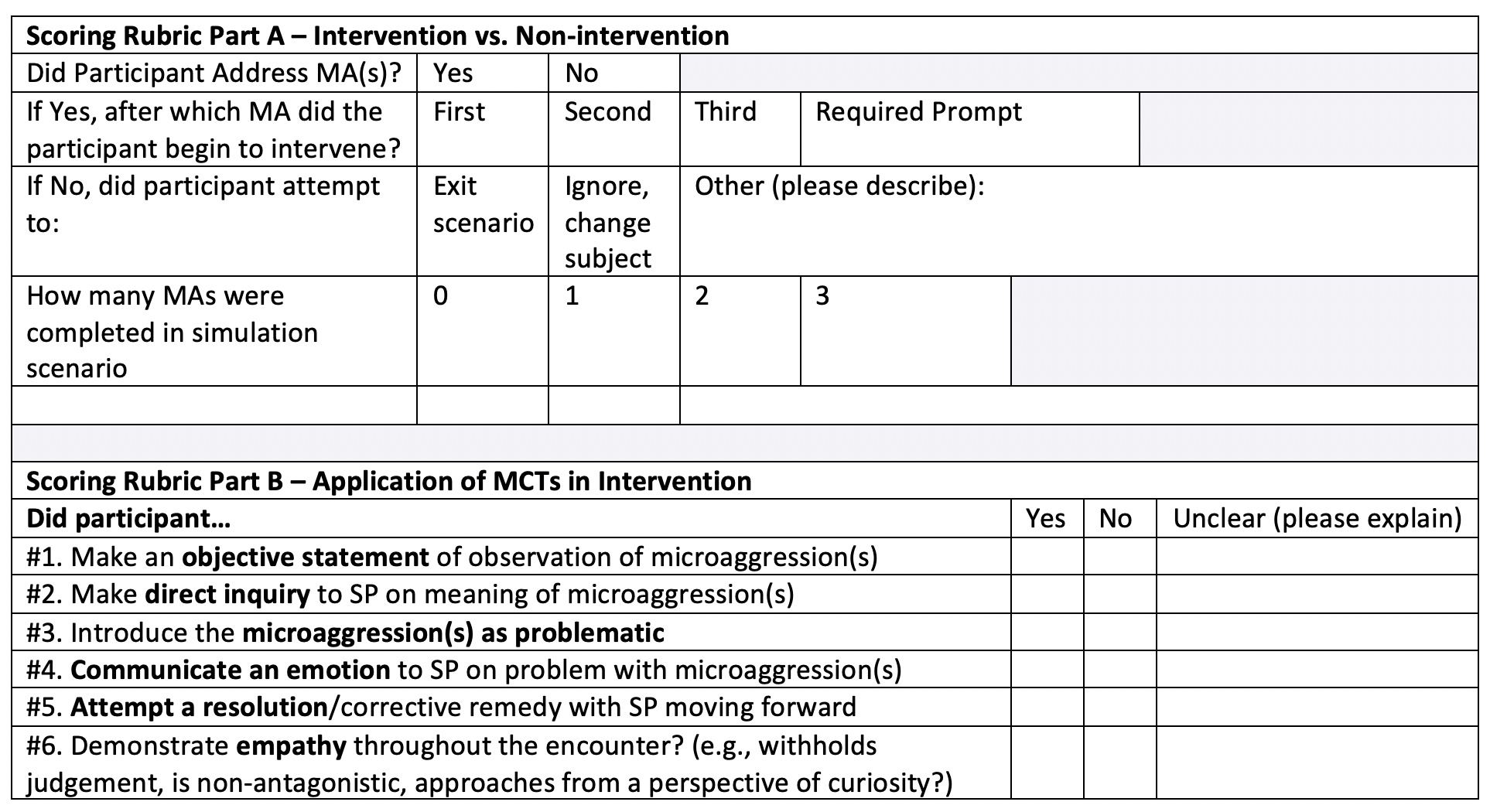
Description: This was a single-center, mixed methods cohort study of pediatric residents who participated in two training sessions over six months. The first session was a didactic presentation on anti-racism and MCTs and the second was an interactive workshop on emotional self-regulation and MCTs. Two groups of residents participated. Group A completed both training sessions and Group B completed only the second training session (Figure 1). In Session 1, residents received didactic education on anti-racism, microaggressions, and three MCTs to address microaggressions as a bystander. In Session 2, residents reviewed the MCTs and completed a workshop highlighting the utility of emotional self-regulation when responding to a microaggression. Trainees practiced responding to racist microaggressions in SPS scenarios, both at the beginning and end of Sessions 1 and 2. These were recorded for later evaluation. With input from other experts, our team developed an observational assessment tool, which measured how the resident responded to the microaggression event and whether any of the six skills of the MCTs given in the training were utilized (Table 1). Pre- and post-training self-assessments were given at each session to measure change in knowledge and confidence over time. Preliminary data showed variation in improvement between MCT skills. Overall, trainees in both groups (A and B) consistently demonstrated “Empathy” in all scenarios, pre- and post-assessment. They made similar improvements in use of “Objective Statements” and “Direct Inquiry” after both training sessions (1 and 2). In Group A, there was a large increase in “Communication of Emotion” after Session 1 (∆52%), but only a 4% change after Session 2, with a large decline between sessions. However, there was more improvement in “Attempt a Resolution” in both groups after Session 2 (Group A, ∆40%; Group B, ∆42%) rather than Session 1 (Group A, ∆6%).
Conclusions: SPS is a potentially effective tool for racist microaggression education and training and can be used to measure skill acquisition. While some skills of MCT training are easily performed and improved on by residents in simulation, other skills remain challenging. The addition of emotional self-regulation training may provide added competency to resolve a conflict that is not typically provided in microaggression training. This highlights a need to emphasize cognitive and emotional aspects of communication in microaggression trainings.