Background:
Over the last two decades concerns have been raised about the potential risk of blood transfusion over the benefits. General restrictive red blood cell (RBC) transfusion approach for anemic hospitalized patients (thresh hold of 7 gm %) has been adopted by American hematology society (AHS) in 2012. It is important to recognize that guidelines should be individualized with the patients, and its strict implementation may harm if the physician fails to review the patient comprehensively. Our study aims to look at the trend of blood transfusion in acute gastrointestinal bleeding (GIB) using a large US inpatient database.
Methods:
We used the Nationwide Inpatient Sample (NIS) database for years 2006-2012 to identify adult patients >=18 years of age with acute GIB (combination of International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes 578.0, 578.1, 578.9 for GIB and previously validated procedure clinical classification software (CCS code 68 for endoscopy as a surrogate for acuity). Recipient of blood transfusion were defined based on procedure CCS code 222. NIS is the largest publicly available all-payer inpatient care database in the United States and is sponsored by the Agency for Healthcare Research and Quality as a part of Healthcare Cost and Utilization Project. Data analysis was done using STATA version 13.0 (College Station, TX).
Results:
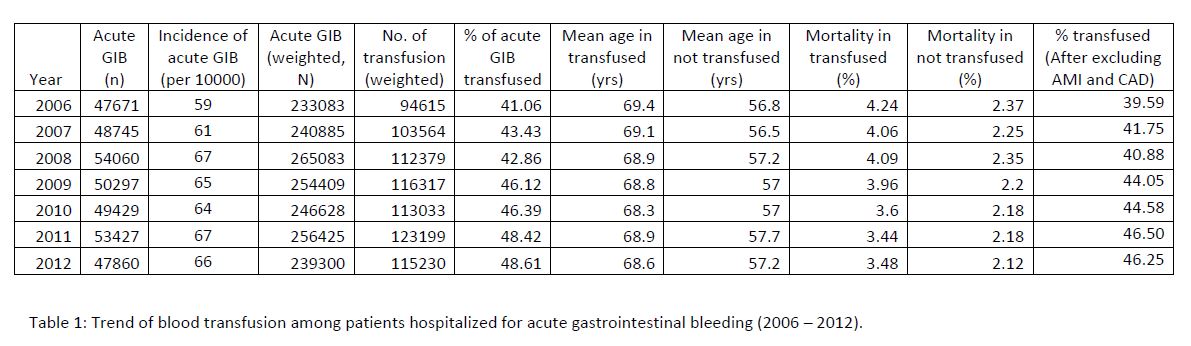
We found 351,489 (weighted N= 1,735,813) adults with acute GI bleed across all years. The proportions of patients with acute GIB who received transfusion showed an increasing trend from 41.06% in 2006 to 48.61% in 2012. Mean age of adults with acute GIB was consistently higher among transfused patients in comparison with those not (p<0.0001) transfused throughout all years. Similarly mortality was consistently higher among adults with acute GIB who received blood transfusion. (Table1)
Conclusions:
Although the concept of restricted blood transfusion started more than two decades ago, it was formally adopted by AHS since 2012. Our study clearly shows increasing trend of transfusion among adult patients with GIB even after excluding patients with myocardial infarction and Coronary artery disease although the latter group had 2% lower rate of transfusion across all year. This is in contrast to the expected decrease in trend with the adoption of restrictive transfusion pattern. This may be due to presentation being more severe secondary to rising use of anticoagulants leading to increase in candidates for restrictive transfusion or persistent GI bleeding or recurrent GI bleeding or overall increasing complex comorbidities requiring higher threshold of transfusion. Analysis including post adoption period data (after 2012) might give more insight regarding the topic.