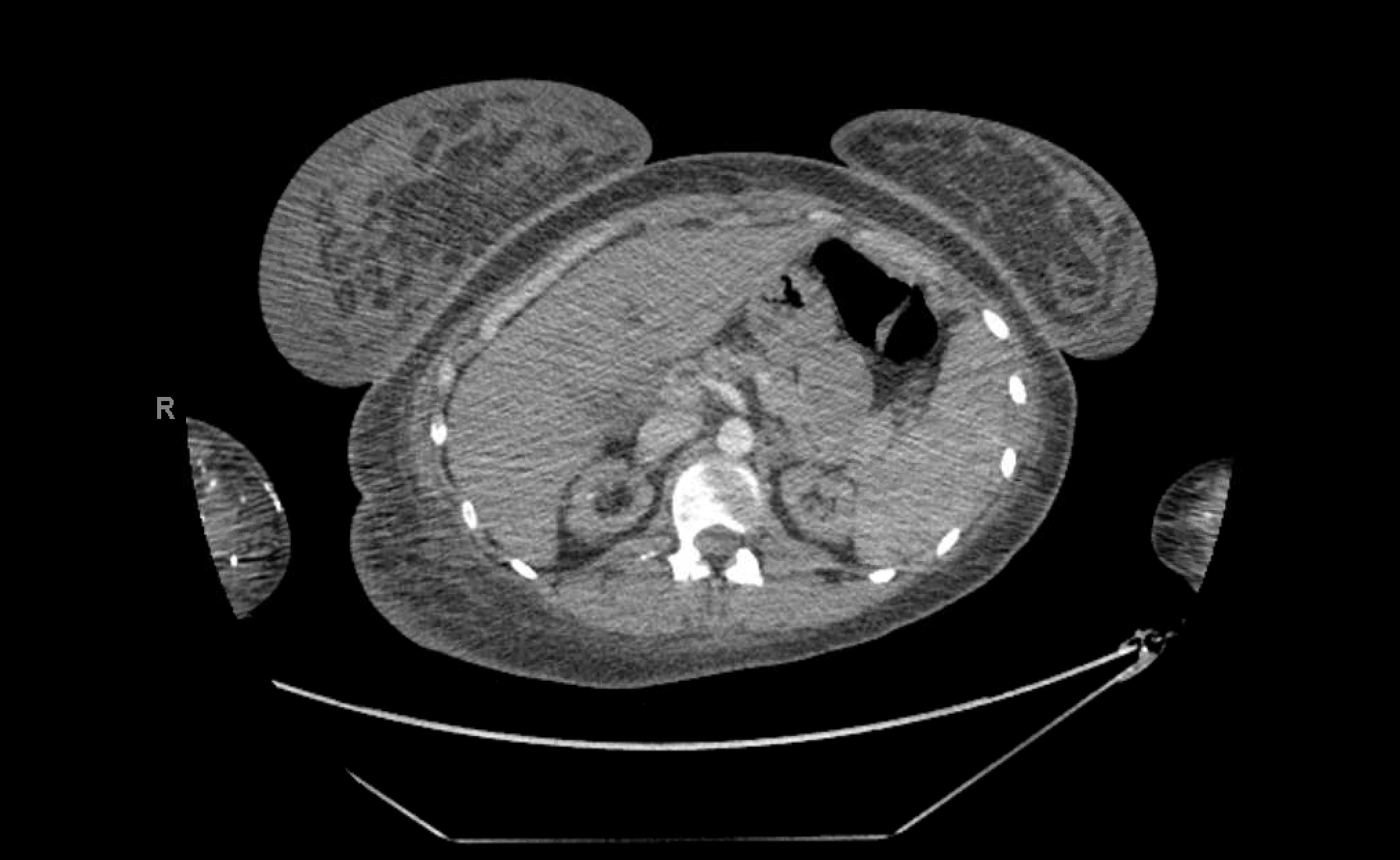
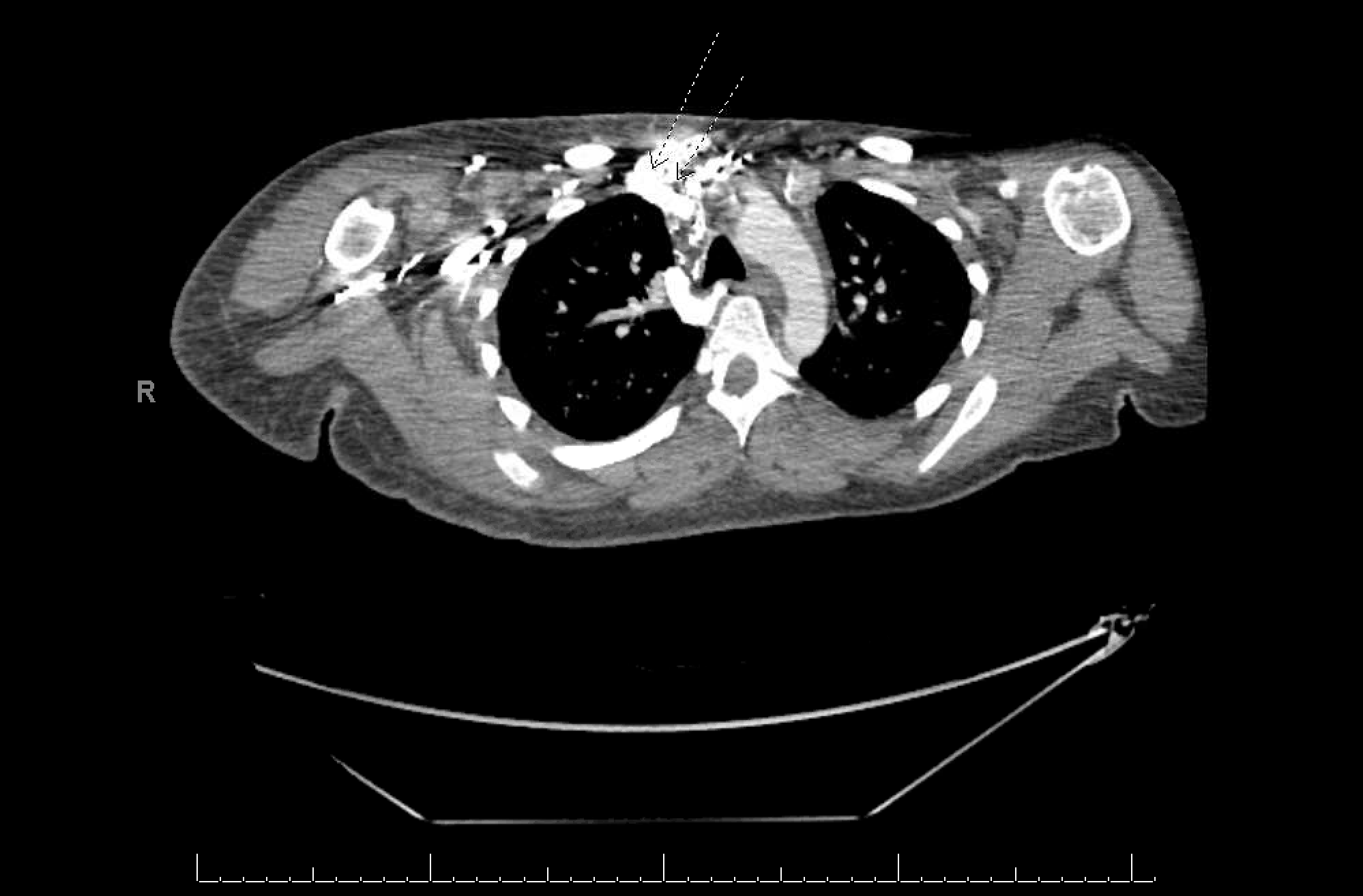
Case Presentation: A 20-year-old female with systemic lupus erythematosus and end stage renal disease (ESRD) secondary to lupus nephritis on hemodialysis via left upper extremity arteriovenous graft presented to the emergency department for pain, erythema, and swelling of the right inferior breast. She was initially treated for cellulitis with resolution of erythema and warmth of skin overlying the right breast. However, she developed progressive swelling of the right breast. Physical exam revealed grossly enlarged and firm right breast. There was diffuse tenderness of palpation but no associated erythema, induration, nipple discharge, or localized fluctuation or mass. Over the following days, the breast became increasingly painful and swelling extended to the right upper extremity. Ultrasound demonstrated skin thickening and edema in the right breast. Duplex was negative for an upper extremity deep venous thrombosis. Subsequent CT venogram revealed an occluded right brachiocephalic vein and multiple collateralized vessels, including the right internal mammary vein, near the right thoracic outlet. CT also demonstrated a right sided pleural effusion. Her symptoms improved with restriction of fluid and salt intake, use of a compression bra, and undertaking multiple daily sessions of ultrafiltration.
Discussion: Central venous stenosis is a known complication in hemodialysis patients following placement of central venous catheters and devices affecting up to 40% of patients and causing significant challenges in terms of future dialysis access as well as other complications.1-7 We present a rare case of young female with right brachiocephalic vein stenosis presenting with atypical right breast swelling. Breast swelling as complication of central venous stenosis is an uncommon phenomenon.8 Our search of the literature yielded three case reports describing breast swelling secondary to subclavian vein stenosis.8,9 Brachiocephalic vein stenosis was implicated in pleural effusion in one case report we revied.5 This is consistent with a right sided pleural effusion incidentally found in our patient. The swelling in our patient was believed to be due to volume overload secondary to ESRD, as well as non-adherence to prescribed fluid and salt restrictions. In the context of these precipitating factors, the atypical swelling can be explained by the excess fluid passing through a narrow collateral internal mammary vein and filtrating into the interstitium and causing expanding edema.
Conclusions: Unilateral breast swelling in a patient with history of central venous catheterization and device placement should raise suspicion for central venous stenosis associated edema and should prompt appropriate investigation and early corrective action.