Background: Discharging complex patients at an academic tertiary care center requires comprehensive evaluation, interprofessional coordination, and meticulous planning to address what is needed to ensure safe and timely discharges. Misalignment across care team members on discharge needs and barriers can lead to a delayed discharge which may result in poor patient satisfaction, increased task burden on clinicians, and inefficient hospital throughput. To strengthen the communication and management of barriers to discharge among team members, we implemented the “Accelerated Discharge Program” (ADP), a Clinical Assistant (CA)-led initiative focused on proactively identifying and resolving discharge-related tasks for patients anticipated to discharge within 24 hours.
Methods: The ADP was implemented in a 600-bed academic Hospital Medicine service with 10 direct-care hospitalist teams managing up to 100 patients daily. A single CA coordinated the program by:1. Sending standardized secure messages Monday through Thursday afternoon to identify patients likely to discharge the following day.2. Confirming outstanding discharge tasks through direct communication with hospitalists.3. Facilitating task completion by engaging appropriate interprofessional team members or addressing administrative duties directly.The CA documented hospitalist-identified barriers to discharge and discharge tasks that the CA assisted with for each patient discussed as part of the ADP. The data collected underwent monthly quality assurance (QA) reviews of the documentation by our clinicians to ensure accuracy and integrity. This included verifying unique patient entries, confirming proper categorization of discharge barriers and tasks, and documenting adjustments with standardized nomenclature. Ambiguities, such as unclear terminology or missing data, were flagged for discussion, while categories were refined for clinical alignment, such as designating “Medical Respite” as “Housing Insecurity.” Adjustments were logged with dates and initials to maintain transparency.
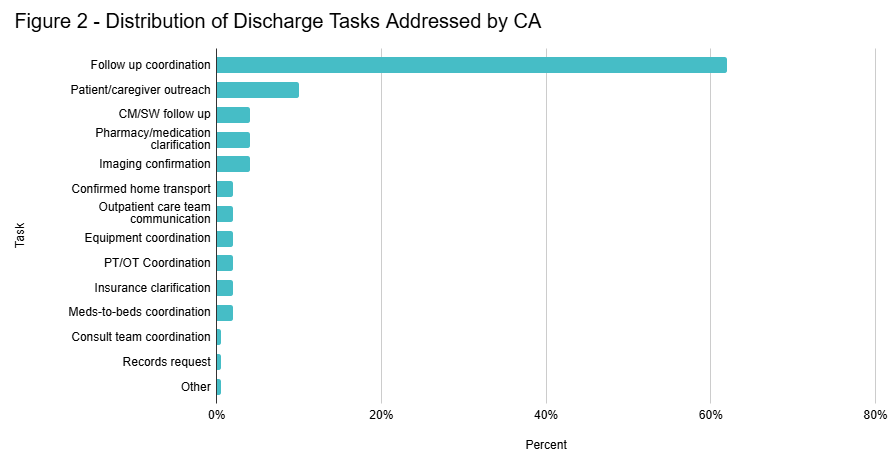
Results: Data were collected over 12 months (October 2023–September 2024), involving 1,002 specific instances in which the hospitalist identified a patient likely to discharge in the following 24 hours. Discharge barriers within 24 hours of expected discharge were identified in 67% of cases, with 61% of this subsegment attributed to acute medical issues and 39% to coordination or administrative barriers. While no action was required in 81% of encounters, the CA directly facilitated task completion in 19%, addressing barriers such as follow-up coordination, patient outreach, and pharmacy clarifications. Figures 1 and 2 illustrate the distribution of barriers and task domains addressed, respectively.
Conclusions: The CA-led ADP initiative effectively identified barriers for patients anticipated to discharge within 24 hours and provided infrastructure to proactively support discharge task completion through interdisciplinary collaboration. By targeting patients nearing discharge readiness, the program streamlined workflows, enabling hospitalists to focus on acute patient care. Future directions include integrating patient and caregiver perspectives in barrier identification and evaluating and incorporating this knowledge into systems-level interventions to address bottlenecks to hospital throughput.