Background: Inpatient diabetes guidelines recommend insulin therapy for persistent hyperglycemia, defined as ≥ 2 glucose values ≥ 180 mg/dL, with a target glucose range of 140–180 mg/dL (1). However, there is no guidance on point of care glucose (POC-G) testing frequency for patients receiving routine four-times-daily tests without meeting persistent hyperglycemia criteria. Our prior study assessed the prevalence and characteristics of low-value POC-G testing (2). Over a 4.4-year period across five hospitals, an average of 45,942 POC-G tests were performed on patients who never received insulin, with 105,686 additional tests on patients not meeting hyperglycemia criteria. In this study, we aimed to develop prediction models using data from the first 48 hours (48h) of admission to identify patients at risk for developing hyperglycemia during their hospitalization, and, conversely, to identify low-risk patients, in whom continued POC-G testing may be of low value.
Methods: The initial cohort and methods have been previously described (2). Briefly, we conducted a secondary analysis of retrospective data from inpatients aged ≥18 years over 4.4 years across five academic and community hospitals, each with at least four glucose measurements. Exclusions included type 1 diabetes, admission glucose >500 mg/dL, home or inpatient use of long/intermediate-acting insulin, ICU admissions, and inpatient use of non-insulin diabetes medications. For model development, we also excluded patients with a length of stay < 4 days, fewer than two POC-G measurements within the first 48h of admission, or any POC-G < 70 mg/dL during that period. We conducted univariate analysis to identify predictors of persistent hyperglycemia (≥2 glucose values ≥180 mg/dL), followed by forward stepwise logistic regression modeling. Model performance was assessed using the C-statistic, sensitivity, specificity, positive and negative predictive values, and likelihood ratios.
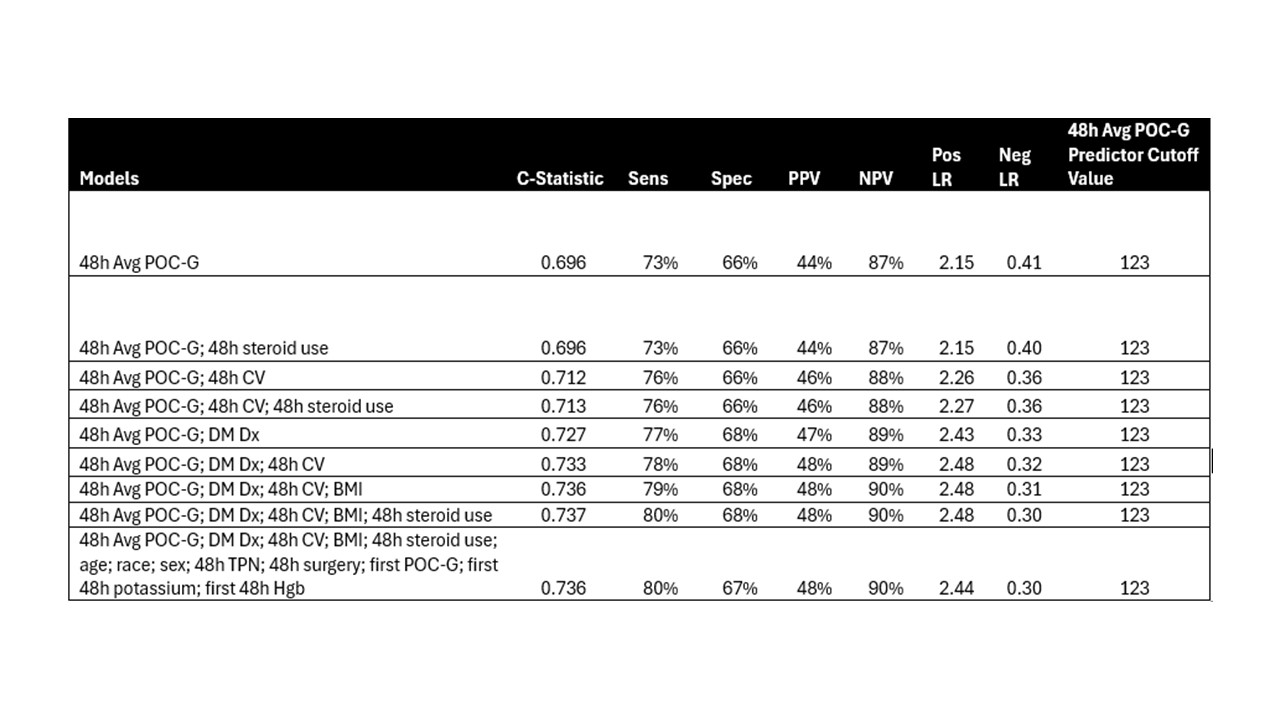
Results: Of 8,244 patients who met the inclusion criteria, 2,205 had ≥2 glucose values ≥180 mg/dL within the first 48h and excluded from model development (Figure 1). Among the remaining 6,039 patients with zero or one POC-G value ≥180 mg/dL during the first 48h, 4,743 (79%) did not meet the guideline definition of persistent hyperglycemia, while 1,476 (24%) developed persistent hyperglycemia in their hospitalization. Several logistic regression models were developed using significant predictor variables identified in the univariate analysis. Models with hemoglobin A1C were excluded due to a high rate of missing data. Table 1 highlights both a comprehensive model incorporating all remaining significant variables and simpler, more practical models, along with their respective performance metrics. Negative results from the models indicate patients who did not meet the outcome of persistent hyperglycemia and would benefit from de-escalation of POC-G testing. Notable model characteristics for identifying negative results include sensitivity of 73% – 80% and negative predictive value of 87% – 90%.
Conclusions: Patient data from the first 48 hours of hospitalization can effectively identify individuals at low risk for persistent hyperglycemia later in their hospital stay, guiding targeted de-escalation of low-value POC-G monitoring. The next steps involve validating these prediction models in an independent patient cohort to select the optimal model for developing a decision-support tool for providers.