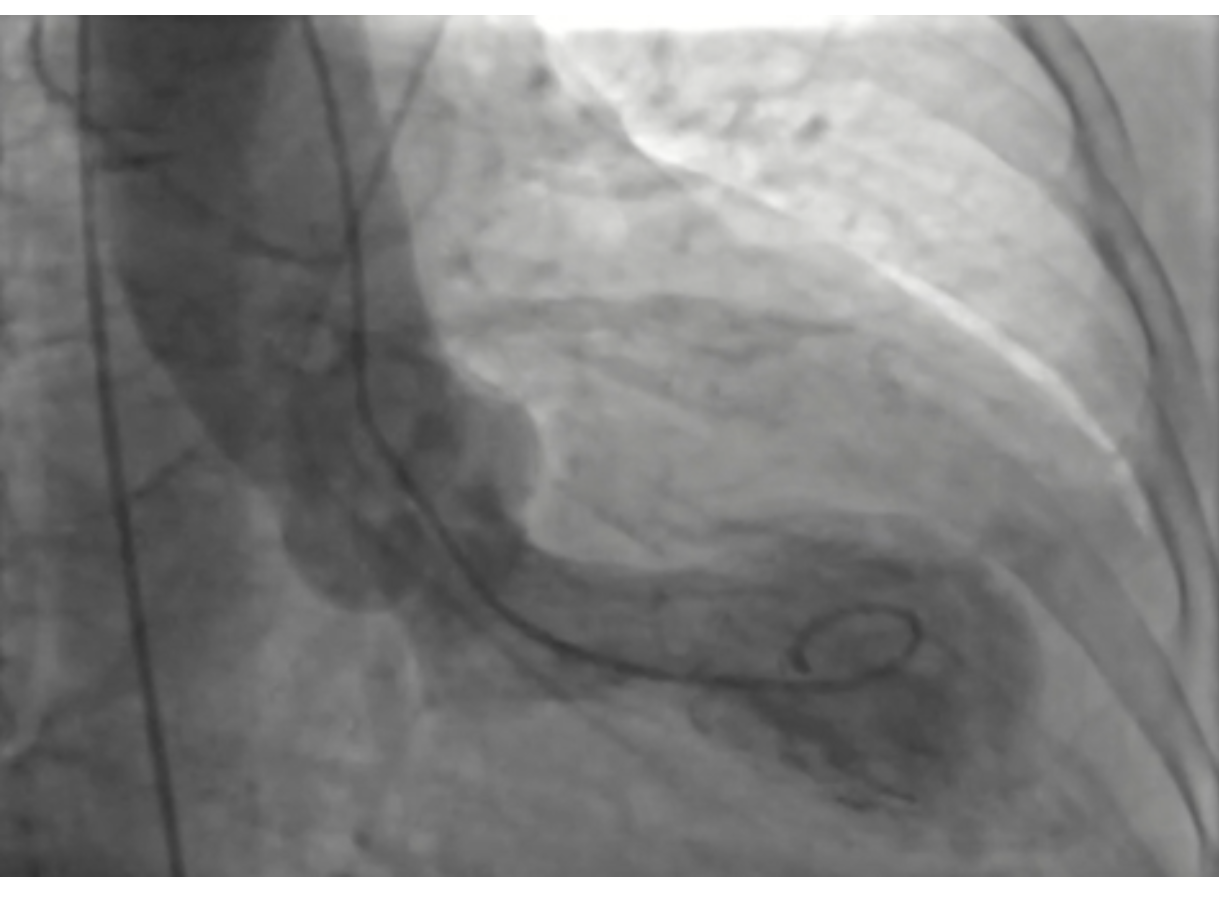
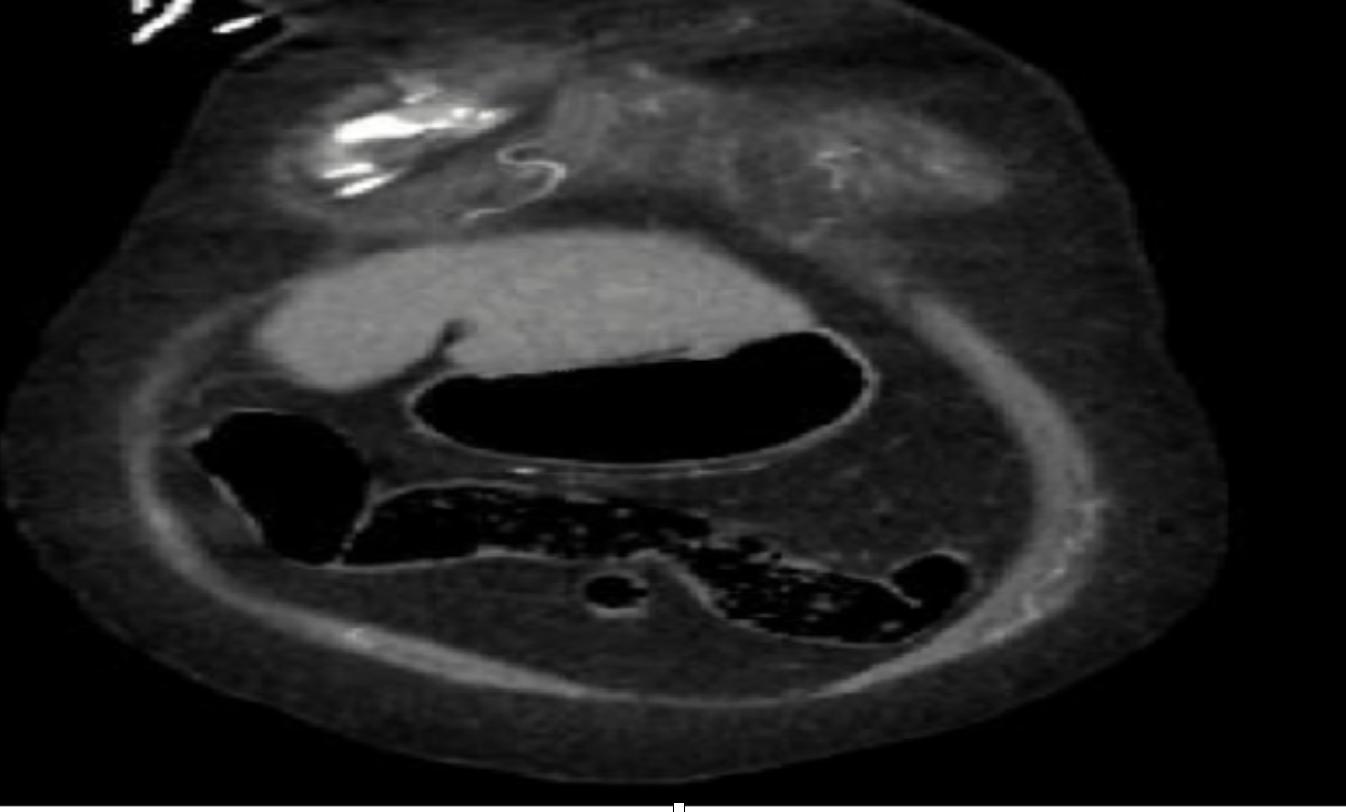
Case Presentation: A 77-year-old female with a history of hypertension and diabetes, presented to the ER with sudden syncope. She reported severe retrosternal chest pain, associated with nausea and vomiting. She stated she has been under extreme emotional stress due to sudden death of a family member. Examination was remarkable for hypotension (70/40 mmhg), cold clammy extremities, faint peripheral pulses, and diaphoresis. The ECG revealed ST-segment elevation in anterior-septal leads. Troponin level was elevated (3.390 ng/ml). Chest x-ray revealed enlarged cardiac silhouette. She was started on vasopressor for cardiogenic shock and underwent emergent cardiac catheterization which revealed non-occlusive coronary artery disease, severe anterolateral hypokinesis, apical dyskinesis, and apical ballooning with estimated LVEF of 20%. Takotsubo cardiomyopathy was speculated.Over the course of the admission, her chest pain persisted which accompanied with severe back pain. The CT chest angiogram showed complex pericardial effusion compatible with hemopericardium. There was extravasation of contrast from the left ventricle into the pericardial space that was suspicious for ventricular wall rupture. The patient underwent emergent cardiothoracic surgery and was found to have left ventricular wall rupture which was repaired. The patient’s condition rapidly deteriorated and went into cardiac arrest. After extensive trials of cardiopulmonary resuscitation, the patient unfortunately expired.
Discussion: TCM has been established as an entity in the past 30 years. Typically, it occurs in middle-aged female as a response to a stressful event, such as bad news, death, or natural disaster. TCM mimics acute myocardial infarction with electrocardiogram changes and elevated troponin.This disorder may be caused by diffuse catecholamine-induced microvascular spasm or dysfunction, resulting in myocardial stunning, or by direct catecholamine-associated myocardial toxicity.
Conclusions: Takotsubo cardiomyopathy (TCM) or stress-induced cardiomyopathy (SICM) is a syndrome characterized by left ventricular dysfunction in the absence of significant coronary artery disease. This disease is usually benign, transient, and is usually treated conservatively with good prognosis. However, rarely it can present with a severe complication of ventricular rupture leading to death. The risk factors for ventricular wall rupture in TCM include female gender, older age, and persistent ST segment elevation. Initial EKG findings of persistently elevated ST-segment in patients with TCM can predict a more serious course of the disease progression and provide a valuable parameter for risk stratification.