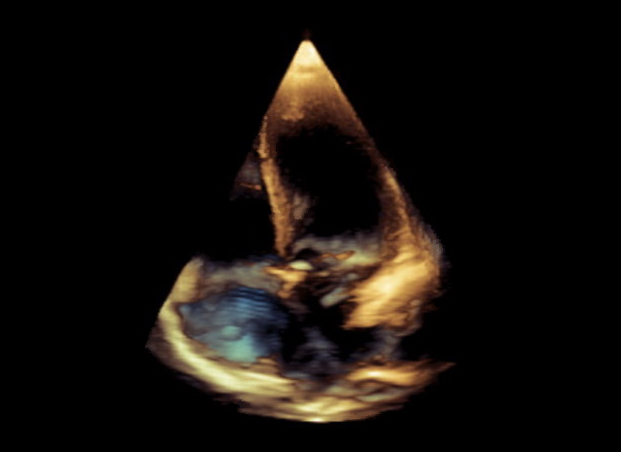
Case Presentation: A 29 year-old woman with sickle cell disease (SCD) on hydroxyurea and L-glutamine, and mild intermittent asthma presented to our institution with right lower extremity and back pain suggestive of a vaso-occlusive crisis. She did not report fever, cough or dyspnea. Vital signs revealed a heart rate of 91/min, blood pressure of 126/86 mmHg, temperature of 36.9 ° C, oxygen saturation (SO2) of 91% on ambient air and a respiratory rate of 15/min. She appeared in mild distress due to pain with anicteric sclerae and dry mucous membranes. There was no JVD; cardiac examination was remarkable for normal S1 and S2 with no murmur. Chest was clear to auscultation bilaterally and right lower extremity was tender to palpation. Laboratory data included hemoglobin of 8.8 gm/dL, WBC count of 8,900 cells/mm3, total bilirubin of 2.1 mg/dL and normal liver enzymes. She received 3 L saline; ketorolac and hydromorphone infusion was initiated. By hospital day (HD) two, her lower extremity pain had resolved. She developed a sharp, midsternal, non-pleuritic chest pain on HD 3, with no associated cough, dyspnea or fever. There was no tachypnea, and SO2 was 87% on room air. Her cardiopulmonary examination was unchanged. Chest radiograph revealed no infiltrate and an electrocardiogram was unremarkable. She had developed a similar episode of chest discomfort associated with hypoxia approximately a month prior, which was evaluated with CT pulmonary angiogram with no pulmonary embolism or consolidation. As her current presentation was inconsistent with acute chest syndrome (ACS) or pulmonary embolism, and due to an elevated BNP (997 pg/ml), contrasted transthoracic echocardiogram (TTE) was obtained. TTE revealed normal LV systolic and diastolic function, normal RV function, trivial tricuspid regurgitation and detection of contrast in the left atrium 5 cardiac cycles after contrast appearance in the right atrium, characteristic of intra-pulmonary shunting. FEV1/FVC was 81% and FEF 25-75% notably 66% on PFT. Budesonide-formoterol by inhaler was initiated with modest improvement in hypoxia.
Discussion: SCD affects approximately 100, 000 Americans and encompasses several clinical syndromes, including vaso-occlusive pain events and stroke. Many patients with SCD develop hypoxia, attributable usually to ACS or pulmonary embolism or pulmonary hypertension. A significant number of patients with hypoxia of unclear etiology are diagnosed with intra-pulmonary right-to-left shunting by bubble-echocardiogram. 1,2 The magnitude of this shunting may exacerbate during vaso-occlusive crisis, 3 and may represent an important mechanism of progressive hypoxia.
Conclusions: In SCD patients presenting with hypoxia, intra-pulmonary shunting should be considered in the differential, especially when the etiology of hypoxia remains unclear.