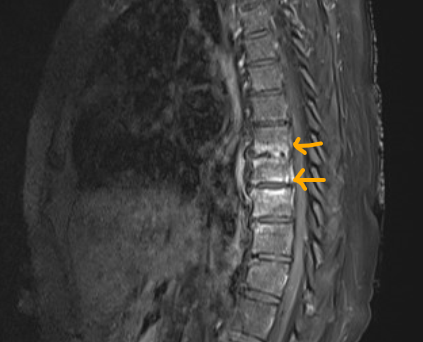
Case Presentation: 87-year-old female presented with chronic low back pain for one month and a new onset fever for 2 days. Patient denied recent travel history, sick contact, chest pain, shortness of breath, urinary symptoms, abdominal pain, diarrhea, or weight loss. She denied lower extremity weakness, sensory abnormality, urinary or bowel incontinence, gait disturbance or other neurological symptoms. On further review, patient reported helping with baby goat deliveries however, denied ingestion of unpasteurized milk. Vital signs were T: 36.5 C, BP: 122/58, HR: 90, RR: 20, SpO2: 97% on room air. Examination revealed alert, oriented female, regular heart rate and rhythm without murmur, normal breath sounds, soft and non-tender abdomen, mild tenderness at lower central thoracic region without swelling or erythema; normal gait, motor and sensory function of bilateral lower extremity and negative straight leg raise sign bilaterally. Initial pertinent laboratory data included WBC 9 x109/L with 57% neutrophils, Hgb 12 g/dl, CRP 1.2mg/L, ESR: 119 mm/h. Urinalysis and a Chest X-ray were normal. MRI T1 post-contrast images of the spine showed enhancement of the T8-T9, T9-T10 vertebral bodies, predominantly the endplates, with mild enhancement of T8-9 disc and prevertebral soft tissue. Patient was empirically started on cefepime and vancomycin. Later, blood cultures grew gram negative coccobacilli in 1 of 2 bottles. Subsequent tests revealed positive Brucella IgM, negative Brucella IgG, and final blood culture positive for Brucella species. Transthoracic Echocardiogram showed normal EF without valvular abnormality. Antibiotics were switched to intravenous gentamicin, doxycycline and rifampicin for 2 weeks, and discharged on oral doxycycline and rifampin to complete a 12 weeks course for Brucella spondylodiscitis.
Discussion: Brucellosis also known as Mediterranean fever, is a systemic disease caused by Brucella species, which are non-motile, intracellular, gram negative coccobacilli and facultative aerobes. Brucellosis is endemic in parts of Asia especially in the Middle east, central and south America and sub-Saharan Africa. Transmission to humans occurs from infected animals (cattle, sheep, goats, camels, pigs), by ingestion of unpasteurized dairy products or by contact with infected tissue or fluids. Brucellosis presents in various forms, depending on severity and degree of organ involvement. Presentation can be mild and nonspecific including fever, night sweats, arthralgias, weight loss, headache, or peculiar to a certain organ system such as back and hip pain (sacroiliitis, spondylitis) to more severe presentations such as endocarditis and meningoencephalitis. Osteoarticular involvement is a relatively common complication with incidence reported at 10-85%. Blood cultures are indicated, even in mild disease with sensitivity up to 70%. Bone marrow cultures is considered gold standard, whereas serology including IgM and IgG antibodies may prove useful (cross reactivity reported with other bacteria). Mild disease responds well to dual therapy of oral doxycycline and rifampin. For moderate to severe disease including spondylodiscitis, IV aminoglycoside (gentamicin) is added to the above regimen for first 2-3 weeks, followed by 6-12 weeks of dual therapy. Prognosis is favorable with relapse rate of 10-15% in osteoarticular involvement, requiring close follow up.
Conclusions: Brucella spondylodiscitis should be considered in the evaluation of low back pain, especially in the endemic regions.