Background: Accurate, high-quality data is critical for work in quality improvement, research, and clinical operations. With an electronic health record (EHR), vast amounts of observational data are collected on patients every day. This data can provide actionable knowledge if an institution can successfully extract and analyze it. At our institution, which adopted the Epic EHR in 2012, there were challenges to obtaining timely and high-quality EHR data, much less being able to use it for quality improvement or research.
Purpose: To develop a Division-level program that could provide high-quality data acquisition and analysis for the ~70+ faculty in the Division of Hospital Medicine.
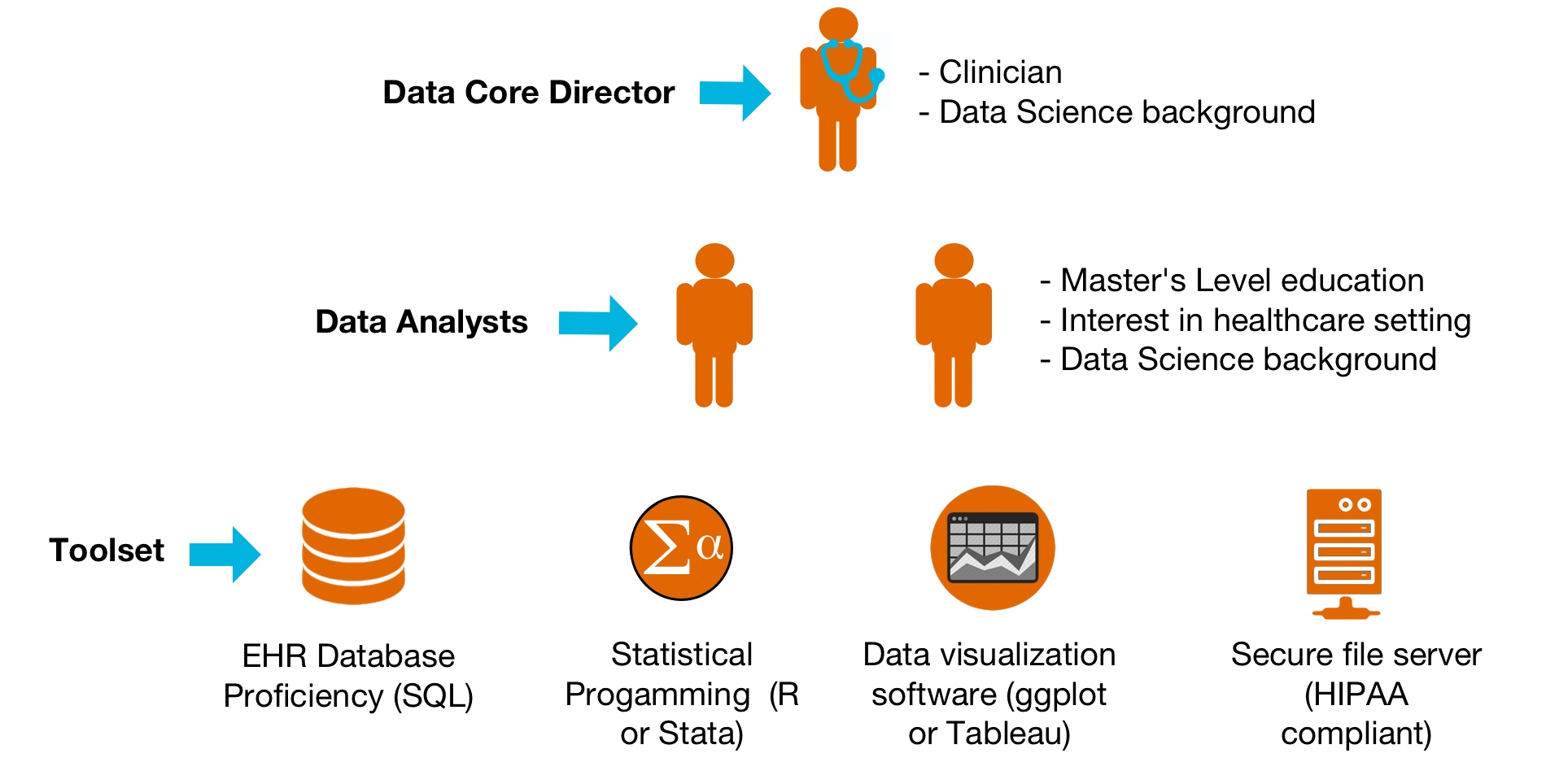
Description: Our Division is based in an 800-bed academic teaching hospital and many faculty are actively engaged in quality improvement or other scholarly projects. In 2016, an initial email survey to faculty found that 86% of respondents reported a need for data and/or analysts in their work. In response, we assembled a working group of divisional leaders in quality improvement, research, and informatics to outline a program that could potentially meet these needs. We subsequently named this program the “Data Core”. We conceptualized the main functions of the Data Core as (1) EHR data extraction; (2) data exploration and visualization; (3) data analytics; and (4) automation of data reports. The group determined that the minimum skill set required to support these functions was: programming in the structured query language (SQL), proficiency in a statistical programming language (e.g. Stata, SAS or R), and certification to use the Epic EHR database. In addition, it was considered vital to include a clinician in Data Core with the expertise to supervise data validation and integrity.
In November, 2016, the Division provided financial support for the Data Core to support a clinician-informaticist and a full-time analyst (Figure). Since its inception, Data Core has provided EHR data that has been used to support 23 separate project requests, which has led to three intramural grants, nine scientific abstracts, and two research manuscripts submitted for peer review. In addition, Data Core provides data to support the Division’s quality metric reports and unit-based leadership team activities.
Conclusions: A divisional Data Core can successfully catalyze the use of EHR data for research, quality improvement, and clinical operations.