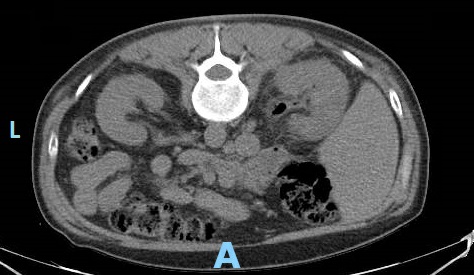
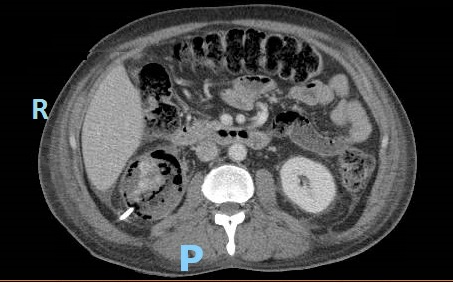
Case Presentation: A 50 year old man with poorly controlled type 2 diabetes mellitus (DM) presented with flank pain, nausea, vomiting, and fever. On exam, he was febrile, tachycardic, hypotensive, and had right sided CVA tenderness. The ER performed a CT stone protocol, however, imaging demonstrated right sided emphysematous pyelonephritis (EPN). Our patient was admitted with severe sepsis, pre-renal acute kidney injury, hyponatremia, and hyperglycemia. Piperacillin/Tazobactam was started, appropriate IV fluid resuscitation was administered, and urology was consulted. Urology recommended placement of both a Foley catheter and percutaneous nephrostomy tube for maximal drainage, even though there were no signs of obstruction. Interim lab work demonstrated a hemoglobin A1c of 16%, increased from 12%. Three days later, despite stable blood pressures and blood and urine cultures demonstrating antibiotic sensitive E. coli, he continued to have a rising leukocytosis, tachycardia, and severe pain. Repeat CT abdomen/pelvis with contrast showed new areas of necrosis and new abscesses in the anterior and lower pole of the right kidney and retroperitoneum. He was taken to the OR for emergent nephrectomy. His course was further complicated by IVC injury and hemorrhagic shock requiring massive transfusion. Subsequent anasarca precluded closure of his abdominal incision and he was monitored in the SICU. He returned to the OR six days later for closure and was discharged home after receiving insulin teaching and DM education.
Discussion: This case highlights the importance of diabetes management in prevention of EPN. Over 80% of patients with EPN have concurrent DM. Our patient’s only risk factor was DM; he had no evidence of obstructive uropathy, was not over age 60, and was not of female sex. Hyperglycemia and glucosuria provide favorable conditions for gas forming pathogens to cause severe infection. DM related autonomic neuropathy results in incomplete emptying of the bladder, further increasing the risk of ascending urinary tract infection. In vitro studies also demonstrate that humoral immunity and neutrophil function are impaired in diabetic patients. This is likely why our patient did not appear clinically worse despite the formation of new abscesses.Management of EPN consists of antibiotic administration and drainage by percutaneous nephrostomy. If these measures are insufficient, total nephrectomy is necessary. CT scan provides prompt diagnosis and staging so appropriate treatment is initiated to preserve renal function and prevent clinical deterioration. CT should be repeated within 3 days if there is concern for worsening infection. Although cases of EPN are fairly rare, its strong association with DM supports the need for optimal glycemic control in our diabetic patients. Additionally, a lower threshold for repeat imaging and escalation of care is warranted in these patients due to their impaired inflammatory response.
Conclusions: EPN requires urgent diagnosis, prompt administration of broad-spectrum antibiotics, and may require surgical drainage or nephrectomy. Most patients with EPN have DM. Consequently, they may have an atypical presentation due to muted inflammatory response, as our patient did not appear severely ill despite worsening of his disease. Glycemic control is important in these patients to prevent and reduce severity of infections. Careful observation is crucial, as patients may not display classic signs of progressing infection.