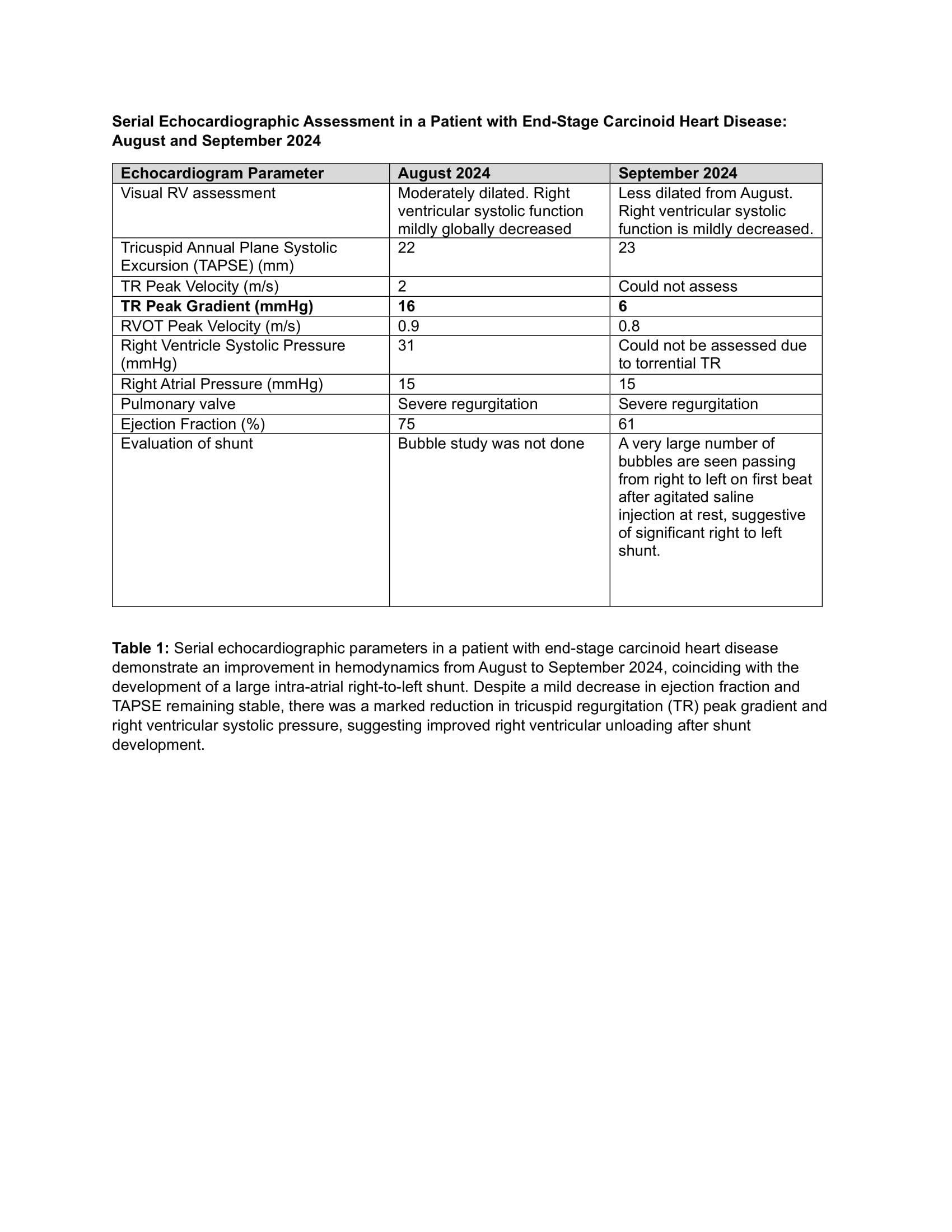
Case Presentation: An 86-year-old male with small bowel carcinoid tumor, complicated by heart disease (CHD), severe tricuspid (TR) and pulmonary regurgitation (PR), right-sided heart failure, atrial fibrillation, and end-stage renal disease on hemodialysis, presented with new-onset dyspnea. His oxygen saturations ranged from 70-88%, improving to 92% with high-flow nasal cannula. Physical exam demonstrated cachexia, pansystolic and diastolic murmurs, and elevated jugular venous pressure. He underwent urgent dialysis, resulting in atrial fibrillation with rapid ventricular response, controlled by amiodarone.Transthoracic echocardiogram revealed an ejection fraction of 61%, a moderately dilated right ventricle with decreased systolic function, and a large right-to-left atrial shunt identified by agitated saline injection. The tricuspid valve was immobile and retracted with torrential TR. There was severe pulmonic regurgitation. The right atrial pressure was 15 mmHg (Table 1). The shunt was new compared to prior echocardiograms, and with its development, the size of the RV decreased.
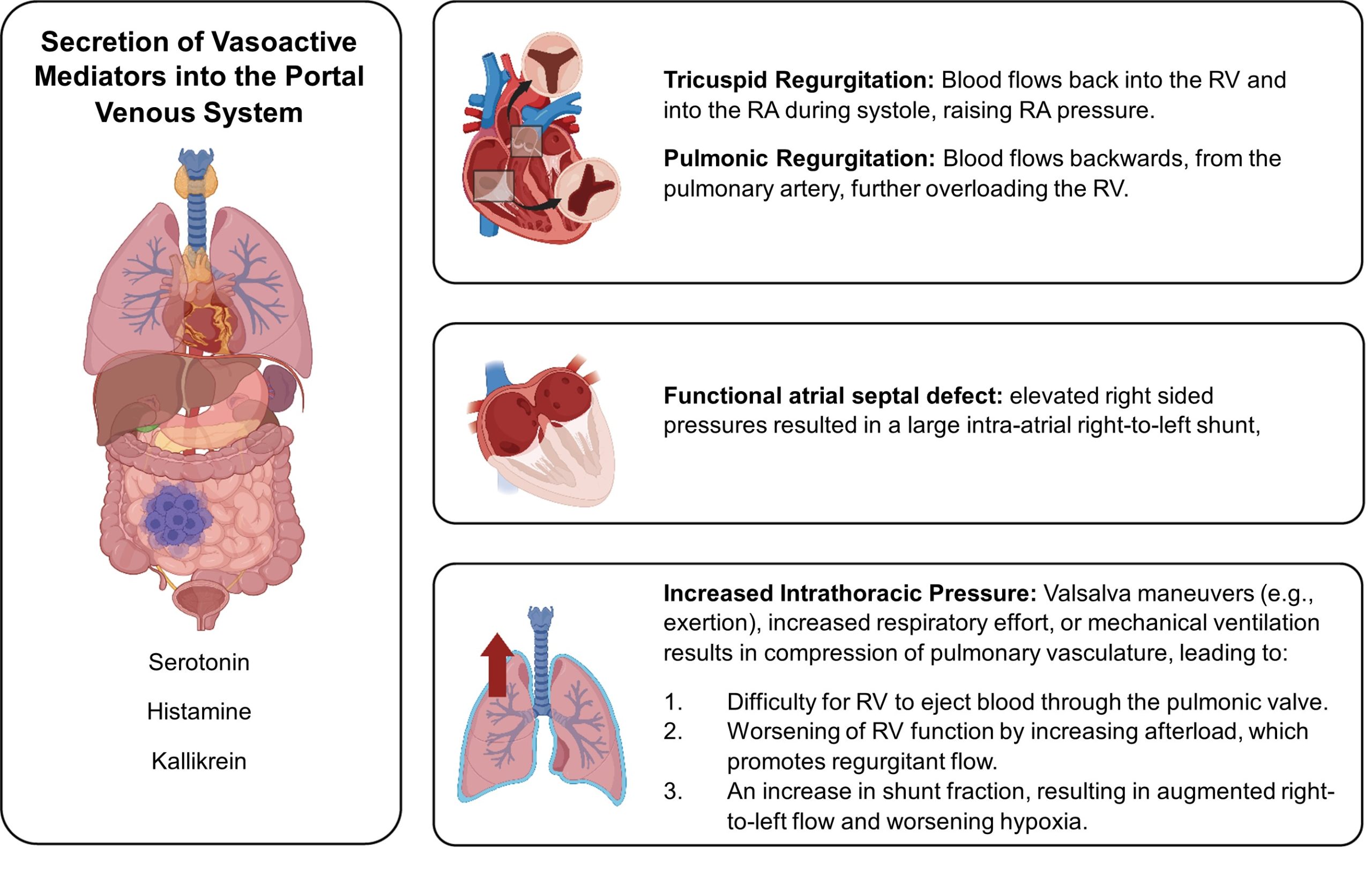
Discussion: Carcinoid tumors, rare neuroendocrine malignancies, secrete vasoactive substances that lead to CHD in up to 70% of patients, manifesting as severe right heart failure, tricuspid and pulmonic valve disease, and interatrial shunts. (1) We present a patient with end-stage CHD, torrential TR, PR, and a large intra-atrial shunt. The etiology of his hypoxia is multifactorial, with key contributors including shunt physiology, worsened by increasing cardiac output and intrathoracic pressure (Figure 1). His TR and PR resulted in right-sided volume overload contributing to significant RV dysfunction, eventually resulting in the development of a functional atrial septal defect which led to platypnea-orthodeoxia syndrome. While children with uncorrected congenital heart disease can tolerate similar hypoxia, this patient’s advanced age limited his physiological reserve. Surgical options, including closure of the atrial defect and placement of IVC valve were considered, but deferred. The focus was shifted from curative interventions to ensuring quality of life through maximizing volume removal, reduction of preload with dialysis, and avoiding iatrogenic clinical decline. The mean life expectancy for CHD is about 1.6 years. (2) Surgical resection and anti-tumor therapies are standard of care. Cardiac surgeries like PFO closure have shown symptomatic relief in some patients with hypoxia and dyspnea.(3) However, in this case, IVC valve placement would increase right-to-left shunt, while closure of the atrial defect without an IVC valve would worsen venous congestion. Still, closure of the atrial defect and placement of IVC valve would result in overt right heart failure due to volume overload given the severe TR and PR, which would worsen with any increase in intrathoracic pressure.
Conclusions: Carcinoid heart disease can manifest as severe right-sided heart failure and valvular dysfunction, leading to complex hemodynamics. Treatment should focus on symptom control, emphasizing individualized, multidisciplinary, and data-driven care, including right heart catheterization and volume management, as key strategies to improve outcomes. Surgical or percutaneous interventions may be considered on a case-by-case basis, with careful attention to each patient’s unique hemodynamic complexities