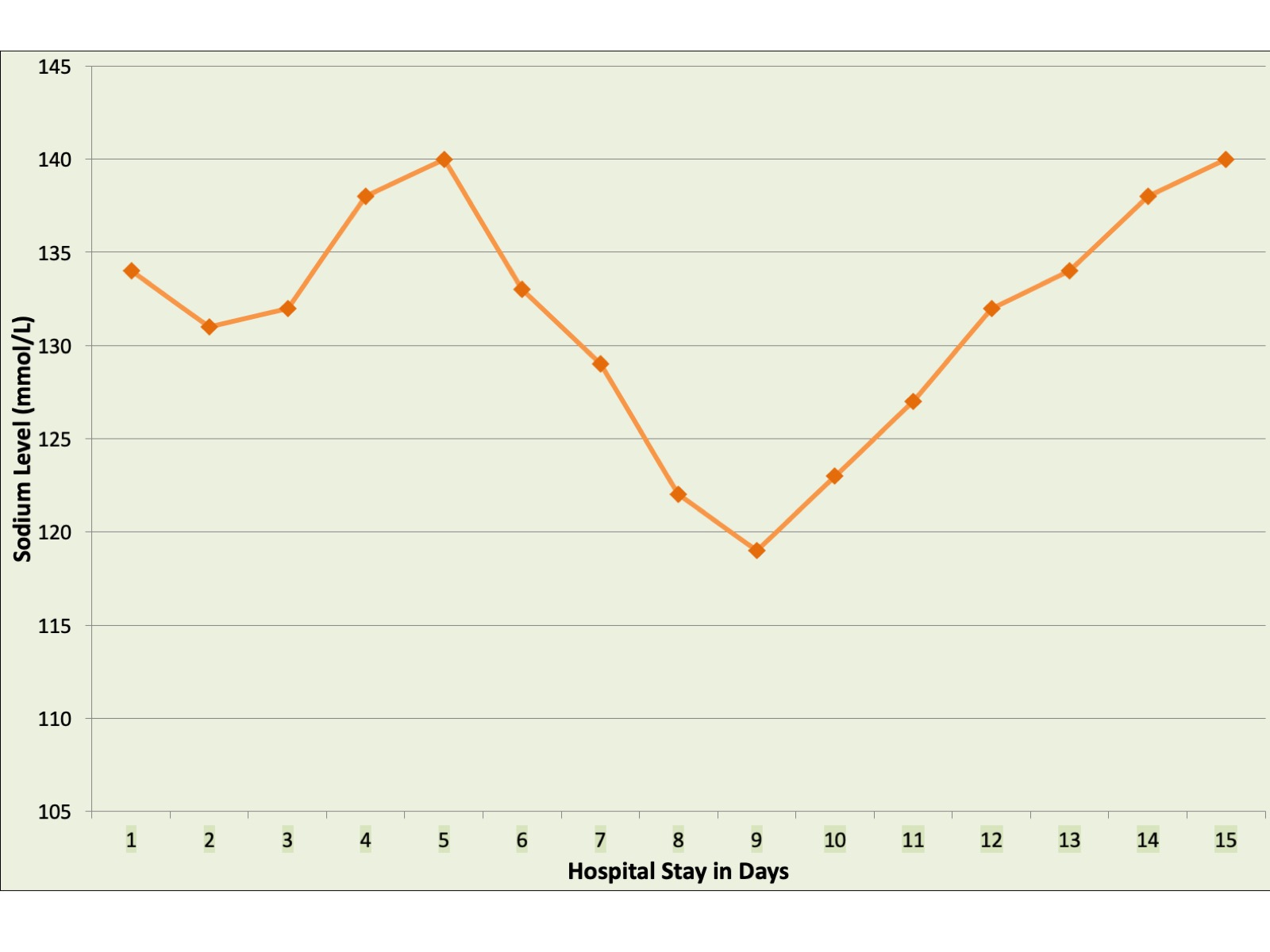
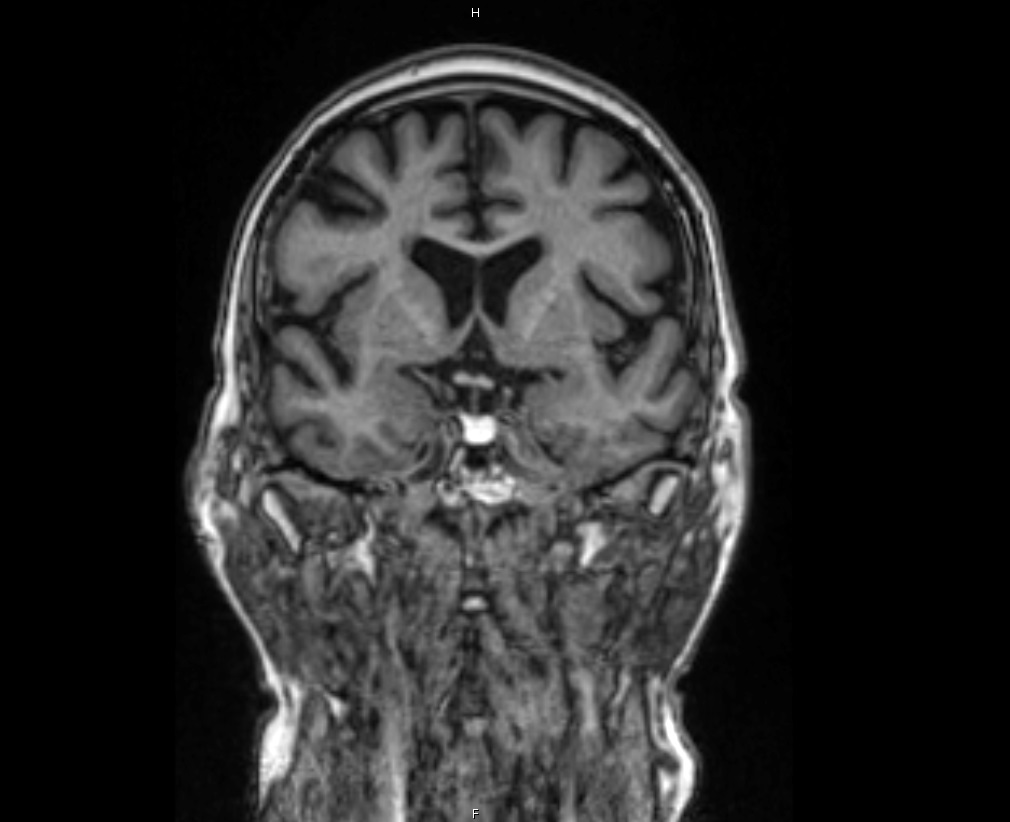
Case Presentation: 72 yo male with history of cerebral artery aneurysm, COPD, and Stage 3 CKD presented to the hospital for elective angiography of a cerebral aneurysm. He developed PEA arrest in the preprocedural setting and ROSC was achieved after 5 minutes of CPR. Patients condition improved initially but prior to planned discharge he developed diarrhea and hyponatremia. The hyponatremia failed to correct with intravenous fluids and reached a nadir of 118 mmol/L (Figure 1). Biochemical work up revealed: Inappropriately high urine Osmolality 516 mOsm/kg (urine Sodium 202 mmol/L), Low Cortisol 0.4mcg/dl, low ACTH 3 pg/ml , Low free T4 0.62 ng/dl, Inappropriately Normal TSH 3.860 mcu/L, low LH, FSH, Total Testosterone, Prolactin and IGF suggestive of SIADH and central hypopituitarism. Endocrinology was consulted and a pituitary MRI was obtained with findings concerning for pituitary apoplexy (Figure 2) in the context of recent cardiac arrest. Neurosurgery recommended non-operative management. Patient was started on cortisol and levothyroxine supplementation. His Sodium and other endocrine parameters returned to normal levels.
Discussion: Pituitary apoplexy is a rare syndrome with an incidence of 0.17 episodes/100,000 person-years. It is precipitated by abrupt hemorrhaging and/or infarction of the pituitary gland, generally in the setting of pituitary adenoma. Although most cases involve macroadenomas, the diagnosis of pituitary tumor remains unknown in more than 75% cases of apoplexy. While cerebral angiography has been previously associated with PA, in our patient the event followed a pre-procedural cardiac arrest.
Conclusions: Pituitary apoplexy may rarely present with subtle metabolic abnormalities. The case reaffirms the fact that there is no substitute for sound clinical reasoning and interdisciplinary collaborative care.