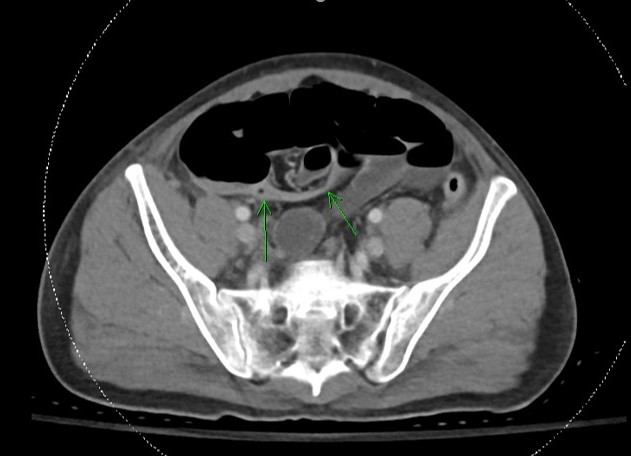
Case Presentation: A 24-year-old man with a past medical history of mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS), malnutrition status-post percutaneous endoscopic gastrostomy (PEG) tube placement, and superior mesenteric artery (SMA) syndrome presented to the hospital with generalized tonic-clonic seizures and severe lactic acidosis. His seizures were treated with levetiracetam, and his lactic acidosis gradually improved over the course of a few days. He then developed severe episodes of non-bloody, nonbilious emesis and obstipation despite an aggressive bowel regimen and manual disimpaction. Gastroenterology service was consulted for further work-up. He remained hemodynamically stable, and his labs were unremarkable except for an elevated lactic acid of 5.7 mmol/L. Computed tomography (CT) scan of the abdomen and pelvis showed distention of small and large bowel loops in addition to decompression of the distal ileum (Image 1), most consistent with an ileus with or without a partial small bowel obstruction (SBO). Patient underwent decompression via nasogastric (NG) tube. After resolution of gastrointestinal (GI) symptoms, patient underwent scheduled PEG tube replacement. Unfortunately, he had recurrent episodes of emesis with tube feeds. Repeat CT scan showed distended stomach without evidence of bowel obstruction or ileus. Total parenteral nutrition (TPN) was started. Upper endoscopy revealed esophagitis, likely from recurrent vomiting. Results were also notable for retained gastric fluid and possible narrowing of the second portion of the duodenum. Small bowel follow-through showed no evidence of high-grade bowel obstruction. Repeated attempts at enteral nutrition resulted in emesis. A third CT scan was concerning for SMA syndrome (Image 2). Patient underwent gastro-jejunal (G-J) tube placement with interventional radiology and was able to tolerate subsequent tube feeds. After several days of close observation, patient was cleared for discharge on G-J tube feeds, with expected improvement in his SMA syndrome after receiving adequate nutrition.
Discussion: While MELAS is classically associated with neurologic symptoms, GI symptoms are also very common and include recurrent vomiting, constipation, and GI dysmotility. A flare of MELAS can further exacerbate GI symptoms and can trigger new symptoms, such as the SMA syndrome seen in our patient. Clinicians should keep a close eye on the caloric intake and weight of a patient.
Conclusions: Clinicians should have a broad differential when evaluating gastrointestinal symptoms, which may be nonspecific, in MELAS patients, as well as in the general population, as there may be a risk for missing treatable diagnoses.