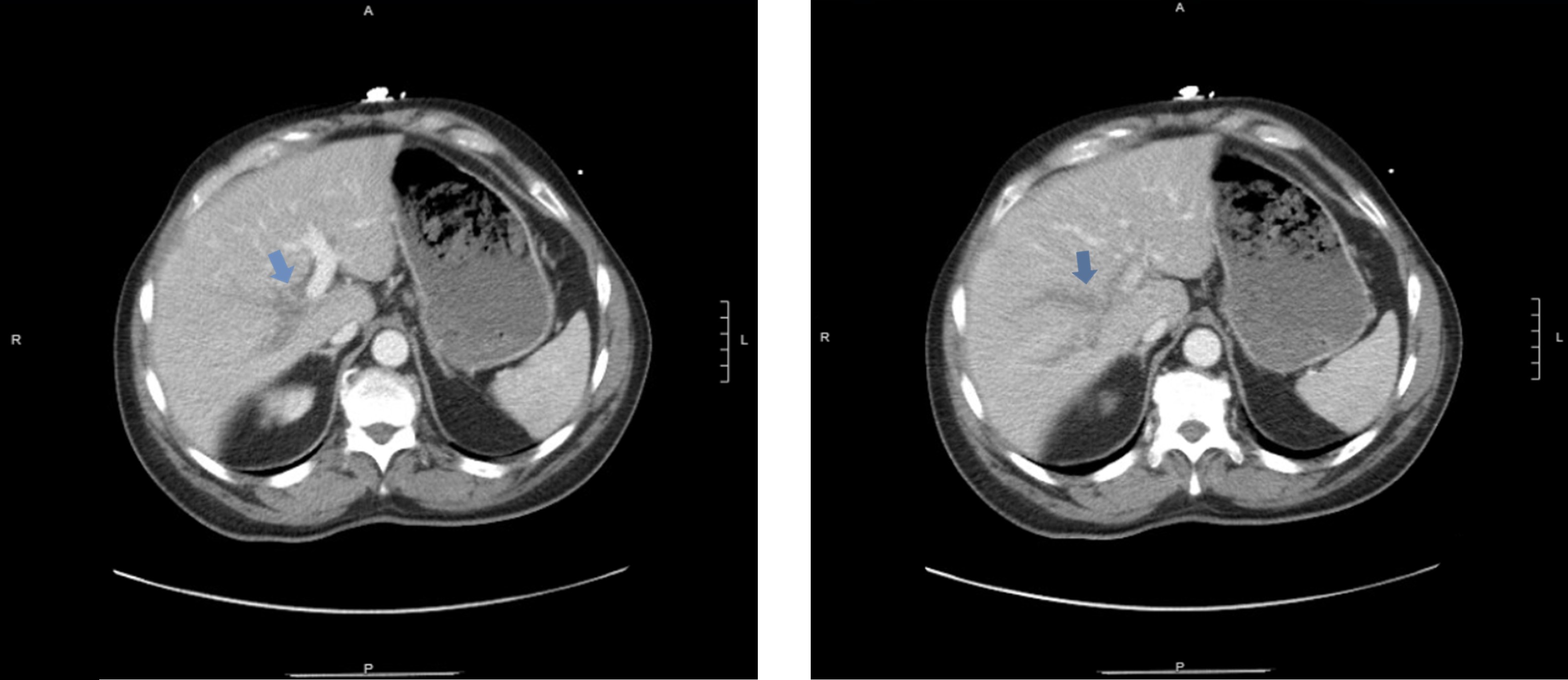
Case Presentation: A 71-year-old male with recent history of gallstone pancreatitis and no known liver disease or malignancy presented with epigastric pain, nausea, and vomiting. Laboratory evaluation revealed lipase of 66 U/L, mild transaminitis, and negative viral hepatitis and HIV serologies. Contrast-enhanced CT showed interval improvement of pancreatitis, with a new occlusive thrombus throughout the right portal venous system, subsequently redemonstrated on portal venous Doppler ultrasound (PVL). Work-up was negative for antiphospholipid antibodies. In the absence of CBC abnormalities or splenomegaly, testing for myeloproliferative disorders was deferred. The patient was diagnosed with non-cirrhotic portal vein thrombosis (PVT), most likely provoked by recent pancreatitis. Anticoagulation was initiated with a heparin infusion and transitioned to rivaroxaban at discharge. Ten days later, he was readmitted for acute lower gastrointestinal bleeding (LGIB) while on rivaroxaban, complicated by acute blood loss anemia. Colonoscopy revealed pan-diverticulosis and internal hemorrhoids without an active bleeding source. PVL showed persistent occlusive right PVT. Vascular surgery determined he was not a candidate for thrombectomy. Rivaroxaban was switched to a titratable heparin infusion, which was briefly held but later resumed given stable vital signs and hemoglobin. He was discharged on reduced-dose apixaban (2.5 mg twice daily) to balance bleeding risk while continuing treatment for PVT.
Discussion: Portal vein thrombosis (PVT) is the formation of a thrombus within the portal venous system, which may extend into the splenic or superior mesenteric veins. In non-cirrhotic patients, PVT is rare. PVT is classified as recent (< 6 months) or chronic (>6 months), with management differing by type. Our patient had a recent PVT, which is the focus of this discussion. Risk factors for non-cirrhotic PVT are systemic (e.g., myeloproliferative disorders, antiphospholipid syndrome, inherited thrombophilias) or local (e.g., hepatobiliary malignancies, intra-abdominal inflammation). Clinical findings include abdominal pain, fever, and ascites. Extension to mesenteric veins may cause bowel infarction. If PVT fails to recanalize, it could lead to portal hypertension. Diagnosis is made by Doppler ultrasound, confirmed with contrast-enhanced CT or MR angiography. Guidelines recommend thrombophilia testing even if a provoking factor is identified. Anticoagulation should be started promptly to facilitate recanalization and prevent thrombus extension, with therapy moderated by bleeding risk. Initial therapy consists of heparin, followed by at least six months of oral anticoagulation, with continuation indicated for thrombophilia or unprovoked PVT. Recent data suggest that direct oral anticoagulants (DOACs) are safe, effective, and may carry a lower bleeding risk, although no randomized trials directly compare them with vitamin K antagonists in PVT. Our case was complicated by LGIB while on rivaroxaban. When bleeding occurs, clinicians must balance re-bleeding risk against thrombus extension, using dose adjustments, close monitoring, or alternative anticoagulation. Accordingly, our patient was transitioned to reduced-dose apixaban, with plans to resume full dose at outpatient follow-up.
Conclusions: Our case offers real-world insight to guide clinicians in managing non-cirrhotic PVT and contributes to the growing evidence supporting DOAC use in thrombosis at unusual sites.
.jpg)