Background: Despite advances in medical education, how modern students engage in experiential learning from patient interactions is not fully understood. Systemic pressures such as healthcare complexities, institutional metrics, and academic demands, leave learners and educators spread thin and frustrated. These prompt students to rely on third-party resources for exam preparation at the expense of direct patient-based learning. Additionally, a growing disconnect emerges between educators’ teaching efforts and students’ learning priorities. In order to clarify how and why this phenomenon occurs, we aim to develop a grounded theory as to how students approach learning on the inpatient wards.
Methods: We analyzed 42 interviews from six student focus groups and 40 resident and attending semi-structured interviews. Using a codebook and consensus coding, we applied constructivist grounded theory with constant comparison, theory memos, and triangulation among investigators, interviewers, and interviewees to generate a process-oriented theory of clinical learning.
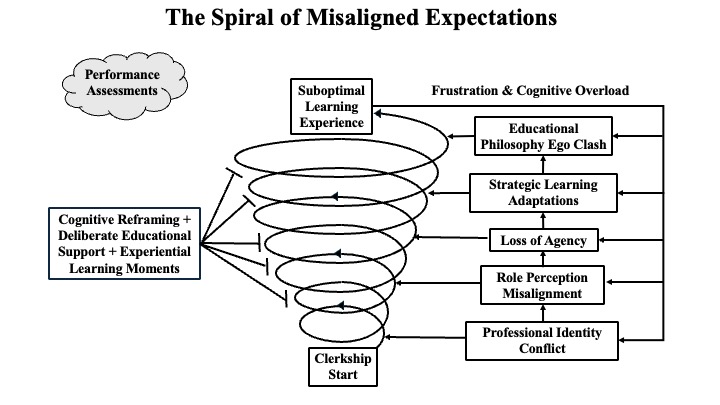
Results: Analysis produced the grounded theory “Spiral of Misaligned Expectations.” Students begin clerkships with a performative mindset shaped by preclinical training, but conflict with growth-oriented roles focused on patient care. Mismatched role perceptions and assessment pressures reduce agency, promoting reliance on question banks and electronic records over direct engagement. This fuels frustration and cognitive overload into a recursive loop of conflict as students, residents, and attendings hold different learning philosophies. Breaking the spiral requires coordinated interventions through educational support, cognitive reframing, and experiential learning as isolated efforts appear insufficient to address these deeply embedded dynamics.
Conclusions: The Spiral of Misaligned Expectations reveals how differing goals among students, residents, and educators create clerkship learning discord. Recognizing this recursive process can guide multi-pronged interventions. Realigning expectations across clerkship, residency, and faculty programs can reduce hidden curriculum harms, support patient-centered education, and keep students engaged at the bedside to enhance learning.