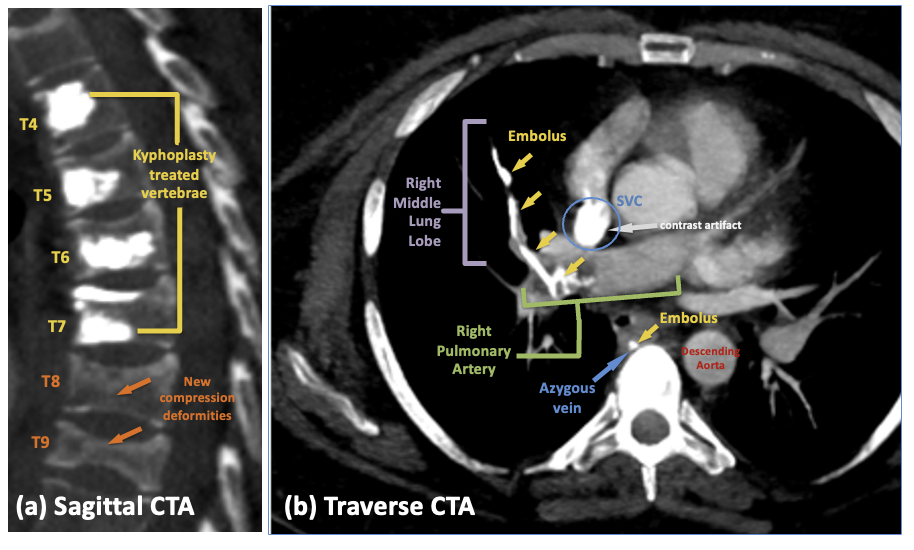
Case Presentation: A 32-year-old female with mast cell activation syndrome, asthma, Ehlers Danlos Syndrome, fibromyalgia, steroid-induced osteopenia and insulin-dependent diabetes presented to an outside hospital with acute on chronic thoracic back pain. There, she underwent kyphoplasty of T4-T7 for thoracic compression fractures and was discharged after a seemingly uncomplicated initial course. She returned 2 weeks later with persistent chest pain, back pain, and dyspnea, and was diagnosed with a pulmonary cement embolism (PCE) of the right main pulmonary artery (PA) with extension into the right middle lobe PA, and azygos vein. After partial mechanical thrombectomy, she was discharged with instructions to continue lifelong anticoagulation. With persistent symptoms of chest discomfort and dyspnea on exertion, she presented to our institution for further evaluation and management. Vital signs: BP 160/99, Pulse 108, Temp 36.4, Resp 20, SpO2 94% on room air. She had normal work of breathing with clear lung fields. Heart was regular, tachycardic, no murmurs, and with jugular venous pressure < 6 cm. Chest exhibited sternal and anterior rib cage tenderness and mid-thoracic spinal tenderness. Repeat imaging redemonstrated the cement thrombi, and a new severe T8 compression deformity. Echocardiogram showed no heart strain. However, due to ongoing symptoms (exertional dyspnea, hypoxemia, chest pain) and risk of long-term complications, thoracic surgery was consulted and performed pulmonary thromboendarterectomy, removing cement material from the affected vasculature.
Discussion: Kyphoplasty stabilizes vertebral fractures using polymethylmethacrylate cement, offering potential pain relief and improved function. cement leakage rates range from 2% to 26%, and symptomatic PCE are rare (0.09% – 0.30% incidence). This case exemplifies the intricate management of symptomatic pulmonary cement embolism in a patient with a complex array of comorbidities. The long-term sequelae of untreated pulmonary cement emboli are not fully understood. Available data suggest untreated PCE can lead to chronic thromboembolic pulmonary hypertension (CTEPH), characterized by persistent high blood pressure in the PAs, resulting in right heart failure and significant morbidity and mortality. Symptoms of CTEPH include progressive dyspnea, fatigue, and decreased exercise tolerance. Additionally, chronic inflammation and granuloma formation around the embolized cement may lead to persistent chest pain and recurrent respiratory infections. Extrapolating previous studies to this case is difficult due to the focus on older populations with osteoporotic fractures or malignancies. The consequences of untreated emboli in younger individuals with complex medical histories remain unclear. Longitudinal studies are needed to develop tailored management strategies for these patients, who may face longer periods of disability or higher long-term risks.
Conclusions: This case underscores the complexities of managing symptomatic PCE in patients with significant comorbidities, highlighting the need for individualized treatment plans and long-term follow-up. Further research is needed to establish guidelines for managing PCE in such cases.