Background: Anemia is an acute and/or chronic condition with a range of underlying etiologies present in an estimated 40-70% of hospitalized patients. While comprehensive diagnostic and treatment algorithms for anemia exist, they are rarely used by hospitalist clinicians in the inpatient setting. This is because these algorithms were derived in ambulatory patients where acute anemia is less common, and because a comprehensive diagnostic workup and treatment of anemia may not be appropriate in patients who are acutely sick with primary diagnoses other than anemia. As a result, there is wide variation in how hospitalists pursue the workup of anemia in hospitalized patients. This is a problem because anemia is a significant risk factor for increased morbidity and mortality and decreased quality of life, and a hospital-based diagnostic and treatment algorithm would be useful for hospitalists and important for mitigating these adverse consequences in hospitalized patients. However, to develop a diagnostic and treatment algorithm, data on the clinically relevant incidence of anemia etiologies in hospitalized patients is needed. Therefore, the purpose of this study was to quantify the distribution of anemia etiologies in hospitalized patients into categories clinically relevant to hospital medicine providers.
Methods: Any hospitalized general medicine patient with a hemoglobin (Hb)< 10 g/dL at any point during their hospitalization was eligible for participation. The clinically relevant anemia categories were derived from laboratory data in consenting patients that was abstracted from the electronic health record (EHR) during the index admission and included: 1) Anemia due to nutritional deficiency including iron, B12, and/or folate deficiency. This group was defined by a ferritin level < 50 ng/mL, or a Vitamin B12 level < 20 pg/mL, or a B12 < 300 pg/mL with a corresponding methylmalonic acid > 0.4 mmol/L, or a serum folate level < 3.4 ng/mL, or a red blood cell folate < 316 ng/mL. 2) Chronic anemia defined by a glomerular filtration rate < 30 mL/min/body surface area or a ferritin > 50 ng/mL. 3) Acute blood loss anemia defined by an admission Hb > 11.5 g/dL. 4) Sickle cell anemia based on a documented history in the EHR and/or an International Classification of Disease 10 code. 5) Undiagnosed anemia was defined in any patient who did not have laboratory values available or meeting criteria for any of the above anemia etiologies. Patients meeting criteria for more than one etiology were categorized as 6) multiple etiologies of anemia.
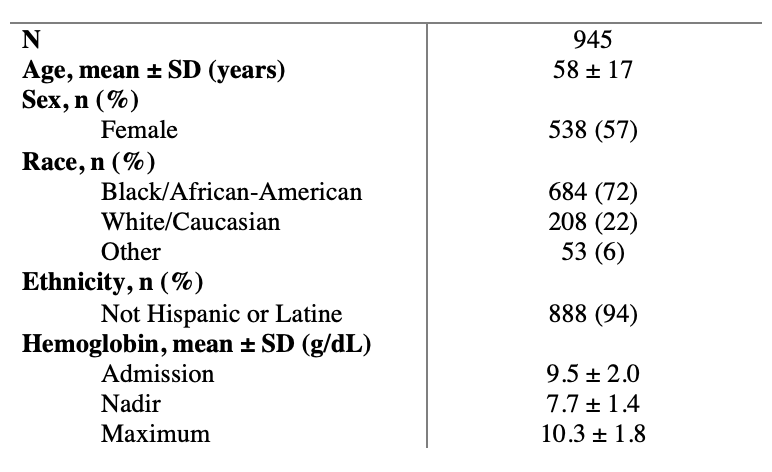
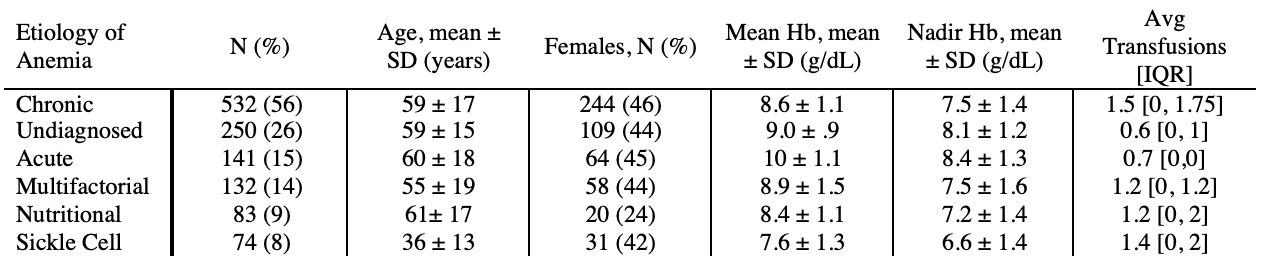
Results: A total of 945 patients consented to the study. Participants had a mean age of 58, 57% were female, 72% were African American, and 94% were non-Hispanic or Latine. The mean admission Hb level of participants was 9.5g/dL, and the mean nadir Hb was 7.7g/dL. Chronic anemia was the most common etiology (532 patients, 56%), followed by undiagnosed anemia (250 patients, 26%), anemia due to acute blood loss (141 patients, 15%), anemia due to nutritional deficiency (83 patients, 9%) and sickle cell anemia (74 patients, 8%). Additionally, 14% of patients were found to have more than one etiology of anemia.
Conclusions: Chronic anemia is the most common etiology of anemia, but a substantial portion of hospitalized adults with anemia have undiagnosed anemia. Overall the distribution of the underlying etiologies of anemia in hospitalized patients differs from the outpatient setting, and this data can be used to develop an optimal standardized approach to anemia diagnosis and treatment in hospitalized patients.