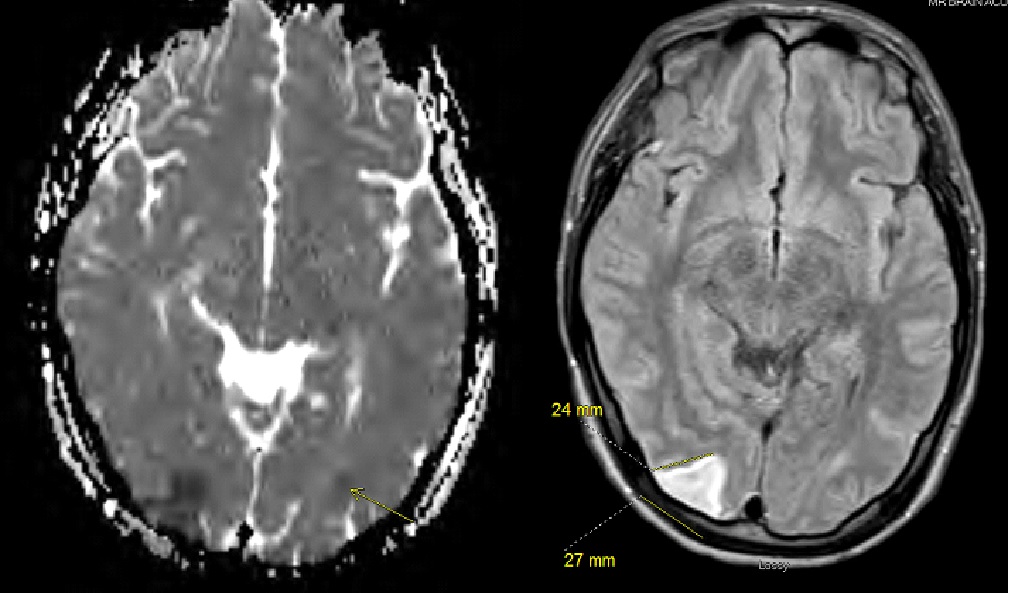
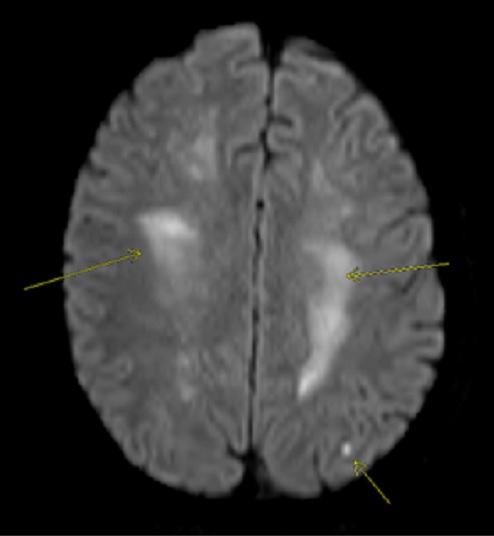
Case Presentation: We present a case of a 20-year old male with past medical history of polysubstance abuse and major depressive disorder who was found unresponsive by his roommate in the morning after black tar heroin use. Roommate injected Narcan without effect and called EMS. Roommate reported both the patient and himself were chronic heroin users. They had recently come across “black tar” heroin from the East Coast and eagerly purchased it due to its lower price compared to that of “white powder” heroin and because it could be safely inhaled, negating the need for risky injection. The patient was hypotensive in the 80s/40s and was intubated for airway protection after demonstrating seizure-like activity and inability to swallow oral secretions. He was started on norepinephrine and taken to the ICU. Neurology was consulted.Significant labs included potassium 5.9 mmol/L, creatinine of 2.3 mmol/L, AST 1134 U/L, ALT 1037 U/L, CK of 1354.7 U/L, PT of 16.2 sec, INR 1.5, and troponin of 1.017 ng/ml. Urine toxicology screen was positive for benzodiazepines, opiates, and cannabis. Neuron-specific enolase reported at 19 ng/ml (reference <15 ng/ml) demonstrating high possibility of anoxic brain injury. Chest CT showed right perihilar consolidation. CT Head did not show acute intracranial pathology but MRI head revealed diffuse leukoencephalopathy with involvement of the bilateral corona radiata, centrum semiovale, and other frontal lobe areas with sparing of the basal ganglia, most of the cortex, and cerebellum. Other findings include a 27 x 24 mm ischemic infarction in the right occipital lobe and a tiny acute lacunar infarction in the left parietal lobe. ECG of the patient demonstrated normal sinus rhythm. Norepinephrine was weaned off by day 2. Patient continued to have tonic-clonic movements despite being on levetiracetam and had to be given midazolam pushes. N-acetylcysteine was given with decrease of LFTs through hospital course.Patient was extubated Day 4; he was able to follow commands slowly and was oriented to place and person but not to time during the day but during the night he would become increasingly confused and agitated requiring reorientation and minor sedation. Roommate reported that this was not baseline. Patient transferred to the regular hospital floor by Day 5. He worked with physical therapy and occupational therapy and improved mentally and functionally.
Discussion: Black tar heroin is a relatively cheaper form of heroin requiring a lower amount of refining and is generally more crude in formation with unknown, varying amounts of impurities. Black tar heroin has been reported to be associated with botulism (1) and necrotizing fasciitis (2) in different case reports via injection. Heroin in general has been reported to be associated with respiratory depression, cardiovascular damage (3), ischemic non-occlusive stroke (4). The inhaled form (also known as “chasing the dragon”) has been known to be associated with spongiform leukoencephalopathy (5) that generally spares the frontal lobes (6).
Conclusions: This case is significant for frontal lobe involvement and multiple ischemic infarcts with the inhalation of black tar heroin as well as subsequent cardiovascular collapse leading to multiorgan damage. Because black tar heroin is cheaper than white powder heroin, it is likely that it will be more widely consumed and medical professionals should be vigilant of the potential sequelae and complications from black tar heroin overdose.