Case Presentation:
51 y/o male with history of hypertension and substance abuse (alcohol, marijuana and tobacco) was found unresponsive lying down in a hotel room by EMS and brought to the Hospital. In the ED patient was hypertensive (189/120 mmHg) and tachycardic. Blood pressure was aggressively managed and mental status improved and patient became more alert. He was found to have an anion gap metabolic acidosis, lactic acidosis and significant elevation of liver enzymes ALT at 650 IU/L and AST at 812 IU/L, positive Troponin I and CPK elevation at 5127 IU/L which was thought to be related to muscle injury from an associated fall or a prolonged period of unresponsiveness of unknown duration. He was unable to recall what exactly had happened. His urine toxicology screen was positive for cocaine, opiates and cannabis. He confirmed using marijuana and “pain pills” but emphatically confirmed he had never used cocaine. In the ICU blood pressure was stabilized and patient was treated as NSTEMI with Troponin I peaking at 3.34 ng/mL. Patient also had AKI (Creatinine 3.36 mg/dL). His liver enzymes continue to rise up reaching AST 1434 IU/L and ALT 950 IU/L. Albumin, bilirubins, alkaline phosphatase and INR were within normal limits throughout the hospitalization. Other causes of trasaminitis in the thousands were ruled out. Acute viral hepatitis and autoimmune hepatitis panel were negative as well as his HIV status. Acetaminophen and salicylates were not detected. There were no documented episodes of hypotension. Liver enzymes trended down throughout his stay as well as CPK, Creatinine and Troponin. Patient recalled that his friend gave him a blunt to smoke that he thought had only cannabis but it was confirmed later it also had cocaine. He never consumed cocaine in the past. He was discharged 5 days after admission with significant clinical improvement. At discharge his AST was 116 IU/L and ALT 385 IU/L. One month follow up showed trasaminases back to baseline.
Discussion:
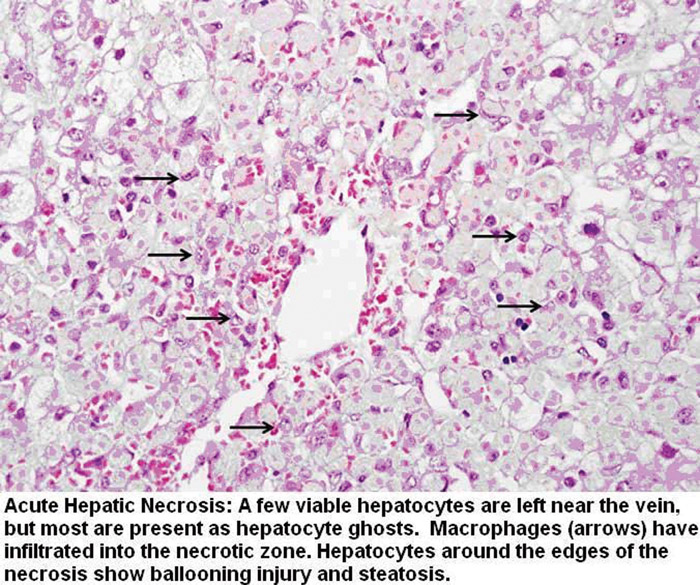
In this case all common causes of trasaminitis in the thousands were ruled out; acetaminophen and drugs toxicity, acute viral, autoimmune hepatitis and ischemic liver injury. We hypothesized that the elevation in liver enzymes was due to cocaine induced acute hepatic necrosis as described in few cases in the literature. The clinical course resembles an acute, toxic hepatic injury with sudden and precipitous onset, marked elevations in serum aminotransferases, and early signs of hepatic dysfunction or failure despite minimal or no elevation of the bilirubins and alkaline phosphatase. Rapid recovery after withdrawal of the agent is also typical. It is usually caused by a direct hepatotoxin and it is dose dependent and “expected”, rather than idiosyncratic. The time to onset is typically short, 1 to 14 days. Strikingly, the serum enzymes usually improve rapidly with stopping the medication, falling by 50% within 8 days. If liver biopsy is obtained (Figure 1) zone 3 coagulative necrosis with scant lobular lymphocytic infiltration, little or no fibrosis or cholestasis and no veno‐occlusive changes are seen.
Conclusions:
The absence of other possible causes of liver injury and the rapid recovery of the hepatic function with evident cocaine use made the case of cocaine induced acute hepatic necrosis. Recovery was remarkable over few weeks demonstrated by his liver function tests back to normal and no evidence of disease at one month follow up.