Background:
Patient care increasingly involves collaborative, team-based approaches in both inpatient and outpatient settings. Optimal transitions of care between the community and the hospital require bidirectional communication and collaboration. This presentation describes a structured, multidisciplinary electronic communication bundle implemented by an academic inpatient service to support care transitions in the management of patients between San Francisco General Hospital (a large, public, urban, teaching hospital) and its partner community primary care health centers in the San Francisco Health Network.
Methods:
Vulnerabilities and inefficiencies were assessed in the existing care transitions framework of the UCSF Family Medicine Inpatient Service, an academic hospital medicine teaching service. Key stakeholders included physicians, pharmacists, social work, behavioral health and clerical staff from inpatient and outpatient care teams. Building on established evidence and stakeholder input, an email-based care transitions bundle was initiated to fulfill three basic functions – facilitate communication, provide actionable patient information and schedule timely follow-up appointments based on estimated date of discharge.
Results:
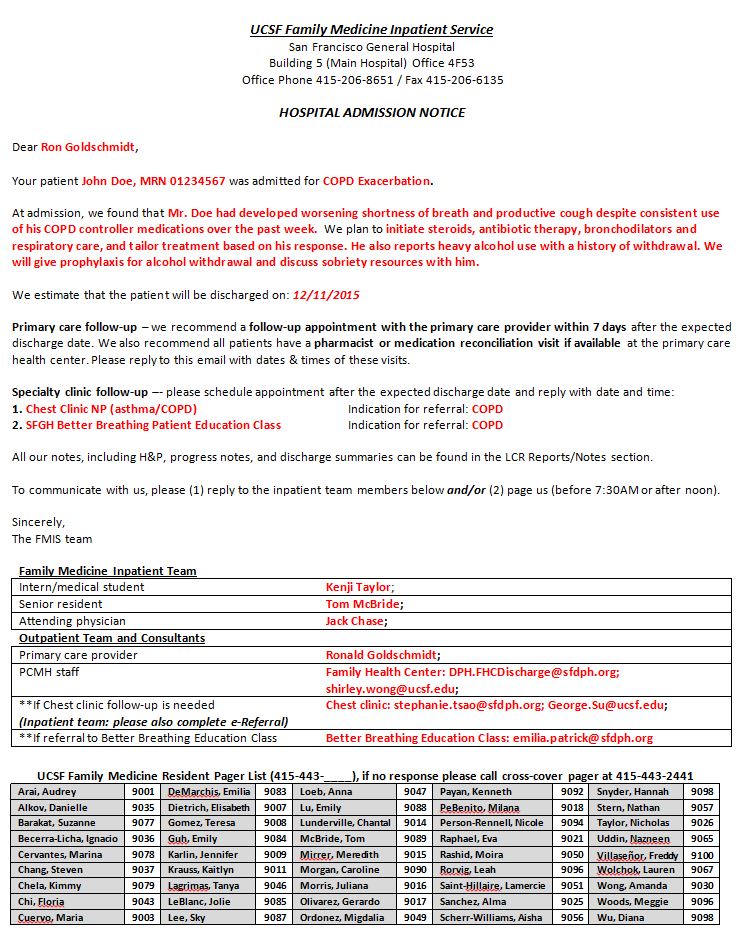
The email-based care transitions bundle, implemented at admission and discharge, includes key information about the patient and circumstances of hospitalization, contact information for inpatient team members, estimated discharge date, referral for follow-up appointments, and critical items for immediate follow-up. The secure email (example in Image 1) connects inpatient and outpatient multidisciplinary team members in a single, HIPPA-compliant communication loop. Sustained improvements were seen in multiple aspects of collaborative care planning over greater than 1500 patient encounters. 94-100% of patients were provided with at least one scheduled follow-up appointment on discharge. 7 day scheduled and attended follow-up appointments increased by 17% and 14% respectively, assiting partner clinics to meet the health system incentive goal for follow-up. When compared with other teaching services also at SFGH not using the email-based system, 8% more patients attended follow-up within 7 days of discharge when care transitions were performed using the email-based bundle.
Qualitative survey of inpatient and outpatient healthcare team members (N = 7/19 and 30/84) showed very positive impacts on efficiency and effectiveness of care coordination. 80% of inpatient housestaff reported increased ease of completion of basic care transitions tasks, spending an average of 50% less time in the process. Large majorities of outpatient providers reported receiving communication within 1-2 days of admit and discharge (86%) and improvements in ease of scheduling post-discharge follow-up (72%), communication with the inpatient team (82%) and ability to meet patients’ multidisciplinary needs (76%). 93% of outpatient providers recommended all services at the hospital adopt a similar system of communication.
Conclusions:
A structured, multidisciplinary, email-based care transitions communication bundle improved rates of scheduled and attended post-discharge follow-up, standardized the method, content and timing of communication between inpatient and outpatient care teams, increased ease and quality of communication and improved provider satisfaction with collaborative care planning.