Background:
Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) is the third leading cause of readmissions and is now included in the Medicare Hospital Readmissions Reduction Program (HRRP). Our institution developed an inter-professional program aimed at reducing all-cause 30-day readmissions for patients admitted with AECOPD.
Methods:
We iteratively developed and piloted our inter-professional COPD HRRP using a quality improvement model from February to September 2014, with full implementation in October 2014. Our program included: an advance practice nurse-led inpatient pulmonary consultation and outpatient one-week follow-up clinic; self-management education (COPD action plan); pharmacy-led medication reconciliation; inhaler technique instruction; a 24-hour patient phone-line; and a nurse-led 48 hour post-discharge call. AECOPD admission was defined by HRRP pre-specified discharge coding guidelines. Patient- and hospital-level demographics were collected by chart review and compared between those readmitted (vs. not) by Chi-squared and Fisher’s exact tests for categorical and independent sample t-tests and Wilcoxin rank-sum tests continuous variables. Healthcare utilization at our hospital within 30 days was obtained by chart review and patient follow-up data.
Results:
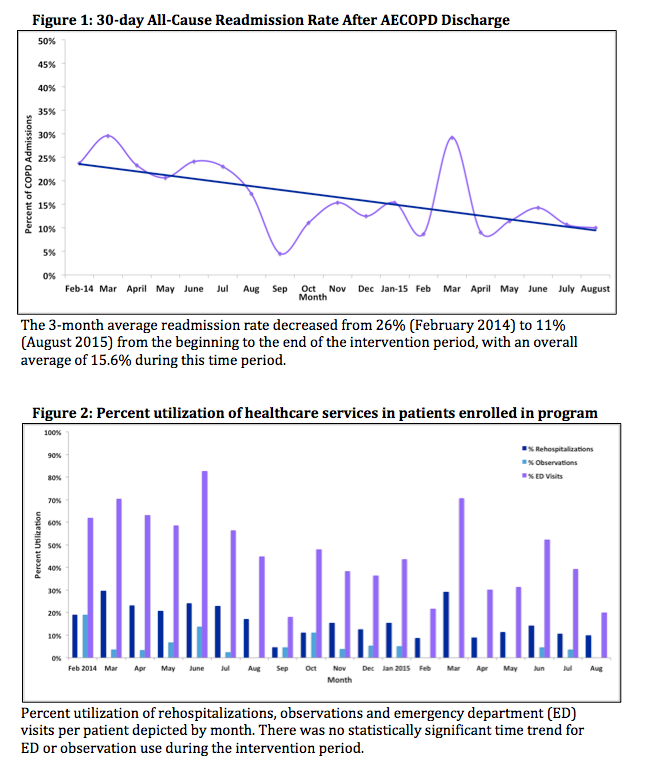
From February to August 31, 2015, there were 583 AECOPD admissions with 91 readmissions within 30 days (15.6%). The majority of patients were female (59%) and black (90%) with a mean age 64 years and median length of stay of 4 days. Respiratory-related diseases accounted for 62% of readmissions; COPD and asthma each accounted for 20%. Cardiac etiologies accounted for 16% of readmissions. The 3-month average readmission rate decreased from 26% to 11% during the intervention period (Figure 1). The median time to readmission or to observation stay was 15 [IQR 6-22] and 8 [IQR 5-19] days respectively. There was no statistically significant increase in utilization of emergency room or observation status during the intervention period (Figure 2).
Conclusions:
Our inter-professional, multi-care setting program demonstrates early success with a nearly 50% reduction in 30-day all-cause COPD readmissions. Median time to readmission was 1.25 times longer compared to national data suggesting a potential benefit of close follow-up within one week. Future analyses planned include a cost analysis and comparisons to historical control data. Our data suggests that a team-based targeted intervention with a comprehensive program can reduce early admissions for AECOPD.