Background: Hip fracture is a common reason for urgent inpatient surgery. In the last few years, several professional societies have identified preoperative echocardiography and stress testing for non-cardiac surgeries as low-value diagnostics. Delaying hip fracture surgery beyond 48 hours leads to worse outcomes. We sought to describe the prevalence of preoperative cardiac testing for inpatient hip fracture repair.
Methods: We used data on hospitalizations for hip fracture surgery between 2011 and 2015 from the State Inpatient Databases of Maryland, New Jersey, and Washington, combined with data on hospital characteristics from the American Hospital Association. The primary outcome was percentage of patients undergoing transthoracic echocardiogram (TTE), stress test, and cardiac catheterization during a hospitalization with a primary procedure code of hip fracture repair. Random effects logistic regression models for each type of test were used to determine which factors might impact test utilization. Random effects were used to account for clustering of testing patterns within hospitals. Covariates included time (3-month intervals), state, age (continuous variable), gender, length of stay, payer (Medicare/Medicaid/private insurance/self-pay/other), hospital teaching status (major teaching/minor teaching/non-teaching), hospital size by number of beds (continuous variable), and mortality score.
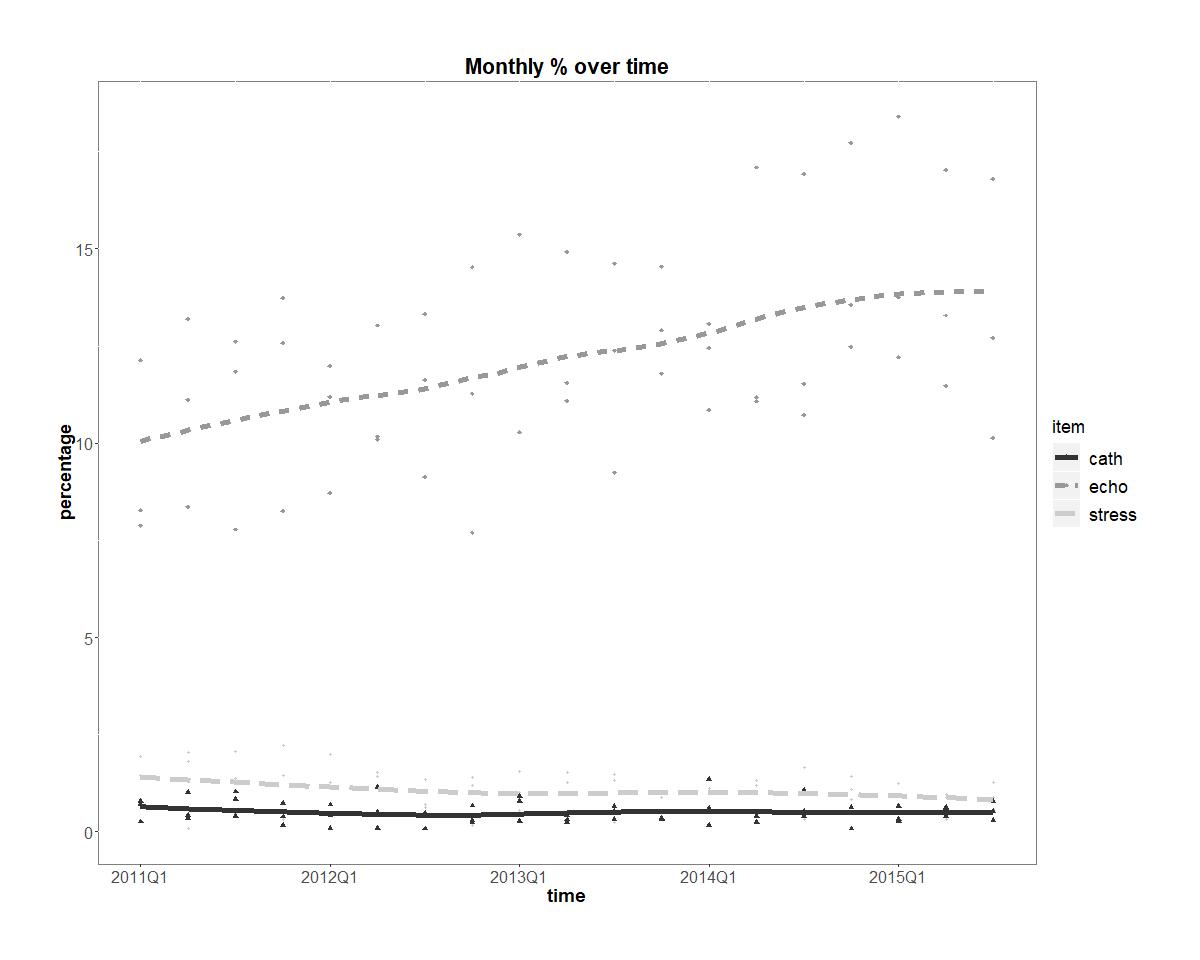
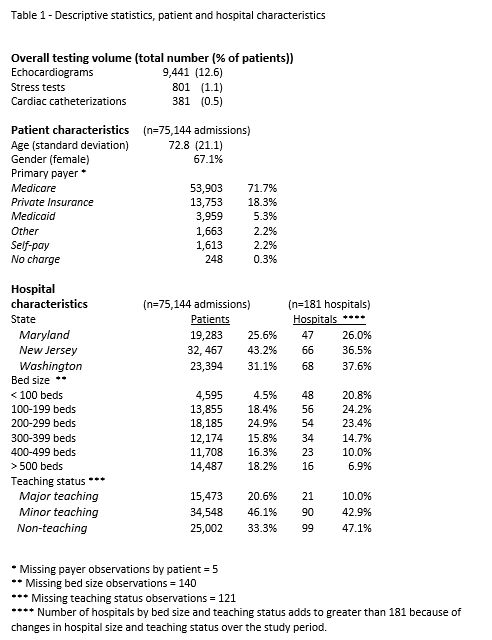
Results: The dataset included 75,144 hospitalizations with a primary procedure code of hip fracture (Table 1). The mean patient age was 72.8 years, and 67% were female. Hospitalizations occurred at 181 hospitals, the plurality of which (42.9%) were minor teaching hospitals. The fraction of hospitalizations which included a TTE, stress test, and cardiac catheterization was 12.6%, 1.1%, and 0.5%, respectively (Table 1). Overall, 13.5% of patients underwent any cardiac testing. The use of TTEs showed a significant increasing trend from 2011 to 2014 (OR 1.04, p<0.0001) (Figure 1).
Conclusions: We found rates of ischemic testing (stress tests and cardiac catheterizations) to be appropriately, and perhaps surprisingly, low. Our results on ischemic testing rates are consistent with previous studies, which have focused on the outpatient setting. The rate of TTEs was higher than in previous studies of the outpatient preoperative setting, though it is unclear what an optimal rate would be. Our findings highlight the importance that quality initiatives focus on true areas of inappropriate utilization. These are the areas in which improvements will have a major impact on healthcare spending.