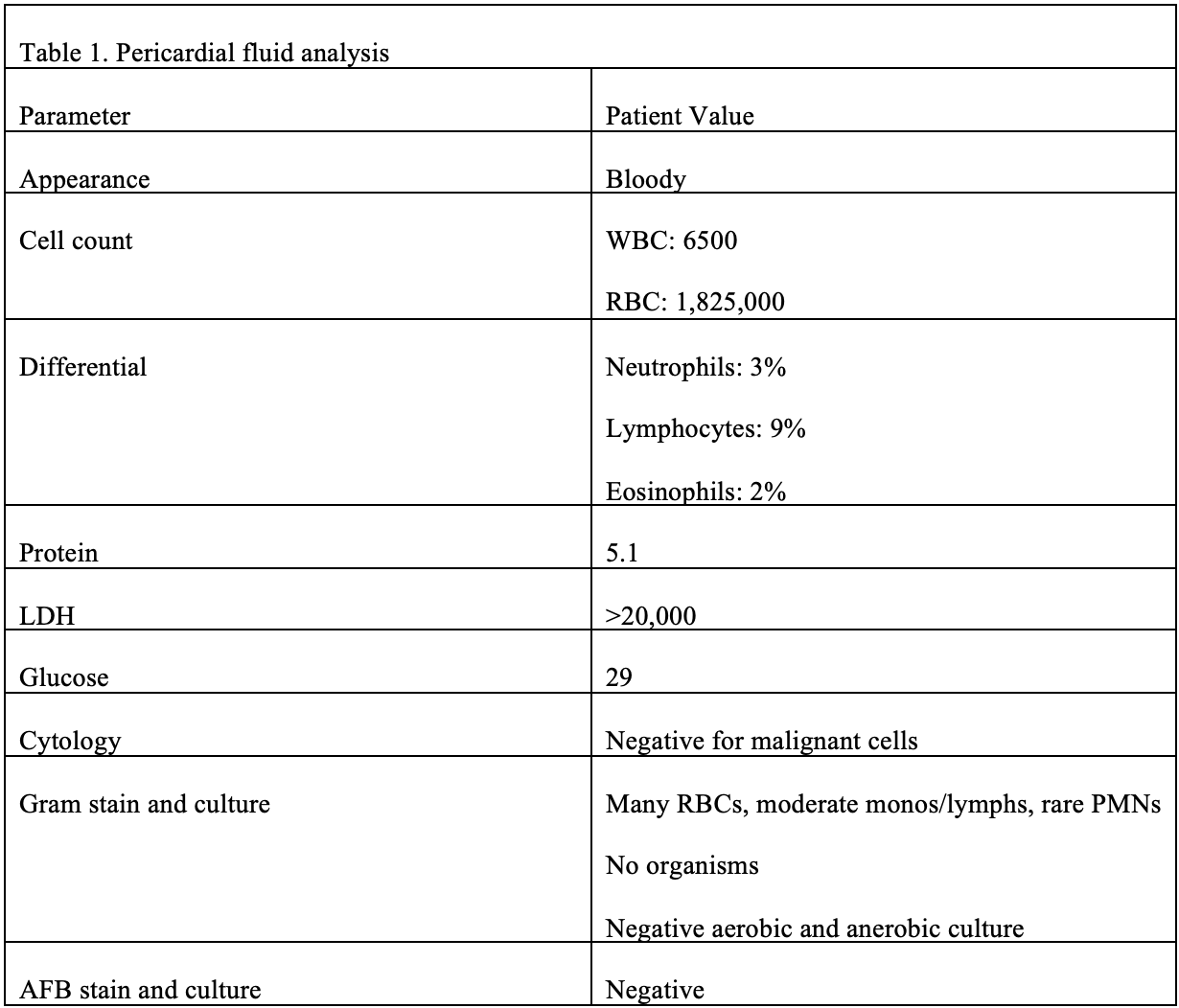
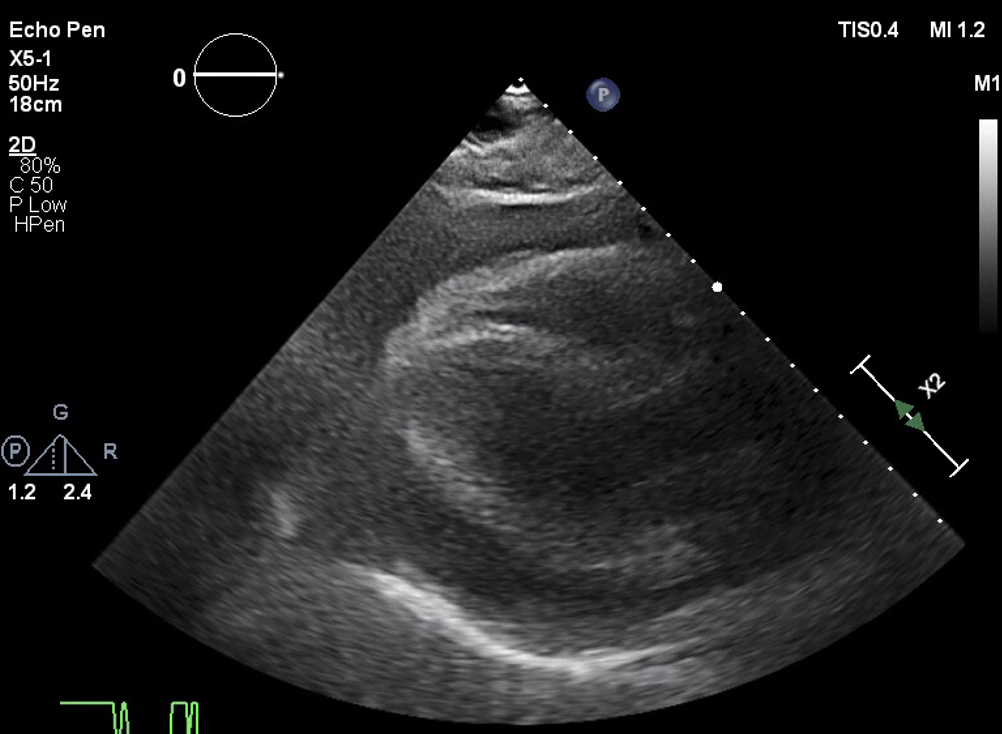
Case Presentation: An 85-year-old male with presumed COPD, tobacco use disorder, hypertension, CKD stage 3, bladder cancer in remission, and BPH presented to the emergency department after a witnessed coughing bout followed by syncope. He had six days of dry cough, rhinorrhea, sore throat, myalgias, dizziness, and dyspnea on exertion and completed azithromycin for presumed bronchitis. COVID and influenza tests were negative. EMS found him hypotensive and in atrial fibrillation with rapid ventricular response (RVR) and gave a 200 ml bolus of normal saline. On admission, BP was 137/85, HR 104 and irregularly irregular, temp 97.7F, RR 20, and oxygen saturation 92% on room air. Exam revealed trace crackles at lung bases, distant heart sounds, normal JVP, and trace lower extremity edema. Labs showed a creatinine of 1.83 mg/dL hemoglobin 9.3g/dL (had dropped from 13g/dL three months prior), proBNP 256 pg/mL, and lactate 1.9 mmol/L; viral panel and blood cultures were negative. CXR demonstrated cardiomegaly and mild pulmonary edema. EKG showed atrial fibrillation with rapid ventricular response and low voltage QRS. He was treated for presumed COPD exacerbation and started on metoprolol for atrial fibrillation. GI evaluated anemia and deferred endoscopy due to lack of overt bleeding. Echocardiography revealed normal biventricular function (EF 66%) and a large pericardial effusion with delayed RV filling in diastole, concerning for tamponade physiology. Emergent pericardiocentesis removed 1.1 L of bloody fluid (glucose 29 mg/dL, protein 5.1g/dL, LDH 20,000 U/L, WBC 6,500 microliters), which was negative for bacteria, AFB and malignant cells. His dyspnea improved, and echocardiograms on day 2 and 3 showed a smaller effusion with resolved tamponade. CT abdomen/pelvis following the pericardiocentesis was negative for obvious malignancy. By discharge his creatinine was at baseline, he had converted to normal sinus rhythm and hemoglobin was stable at 9.6 g/dL. A month later at outpatient follow-up, echo revealed resolved effusion.
Discussion: Syncope accounts for 6% of hospital admissions in the United States [1]. Cough syncope is commonly associated with obstructive lung disease [5]. This patient appeared to have typical cough syncope due to COPD, and pericardial effusion was not considered. In this case, an echocardiogram for new onset atrial fibrillation incidentally revealed pericardial tamponade, a rare cause of cough syncope [2,3,4]. Echocardiography, though not standard in syncope evaluation, is critical when cardiac causes are suspected.Coughing increases intrathoracic pressure, reducing venous return; in tamponade, where preload is already impaired, this can precipitate cerebral hypoperfusion and syncope. Vagal stimulation during coughing can cause peripheral vasodilation and worsen hypotension. Other causes of cough syncope include cardiovascular conditions such as sub-aortic stenosis and constrictive pericarditis, as well as neurologic disorders such as cerebral tumors and hydrocephalus, though most patients also have obstructive lung disease [5]. This case emphasizes maintaining diagnostic breadth in hospital medicine when evaluating syncope in hemodynamically unstable patients.
Conclusions: Cough syncope is typically benign but may rarely signal life-threatening conditions such as cardiac tamponade. Hospitalists should maintain a high index of suspicion for pericardial effusion in patients with cough syncope accompanied by hypotension, arrhythmia, or dyspnea.