Background: Guideline-direct medical therapy (GDMT) improves morbidity and mortality outcomes in heart failure (HF), yet disparities in prescribing patterns persist across insurance types. Previous work at our hospitals demonstrated overall increases in GDMT prescribing following two phases of targeted interventions: financial incentives and education interventions (“Post 1”) and the addition of clinical decision support systems (CDSS) in the EHR (“Post 2”). The extent to which these improvements vary by insurance coverage remains unclear.
Methods: We conducted a retrospective analysis of HF patients stratified by insurance type (Medicaid, Medicare, Private, Uninsured). Patients were divided into two seasonally-matched Pre and Post phases: Pre 1 (7/2023-10/2023) and Post 1 (7/2024-10/2024) and Pre 2 (12/2023-6/2024) and Post 2 (12/2024-6/2025). Post 1 included financial incentives for attendings and educational interventions for all clinicians. Post 2 included the addition of CDSS within novel order sets and HF-specific automated smart phrases. Patients were separated into groups of those who would benefit most from 4-pillar GDMT (HFrEF/HFimpEF) and those who would benefit most from SGLT2i (HFpEF/HFmrEF). Two proportion z-tests were used to assess significant changes in prescribing rates across insurance groups. Relative increases were calculated for all groups. Patients with unknown ejection fraction were excluded. Patients with Veterans’ Affairs insurance were excluded due to the small sample size.
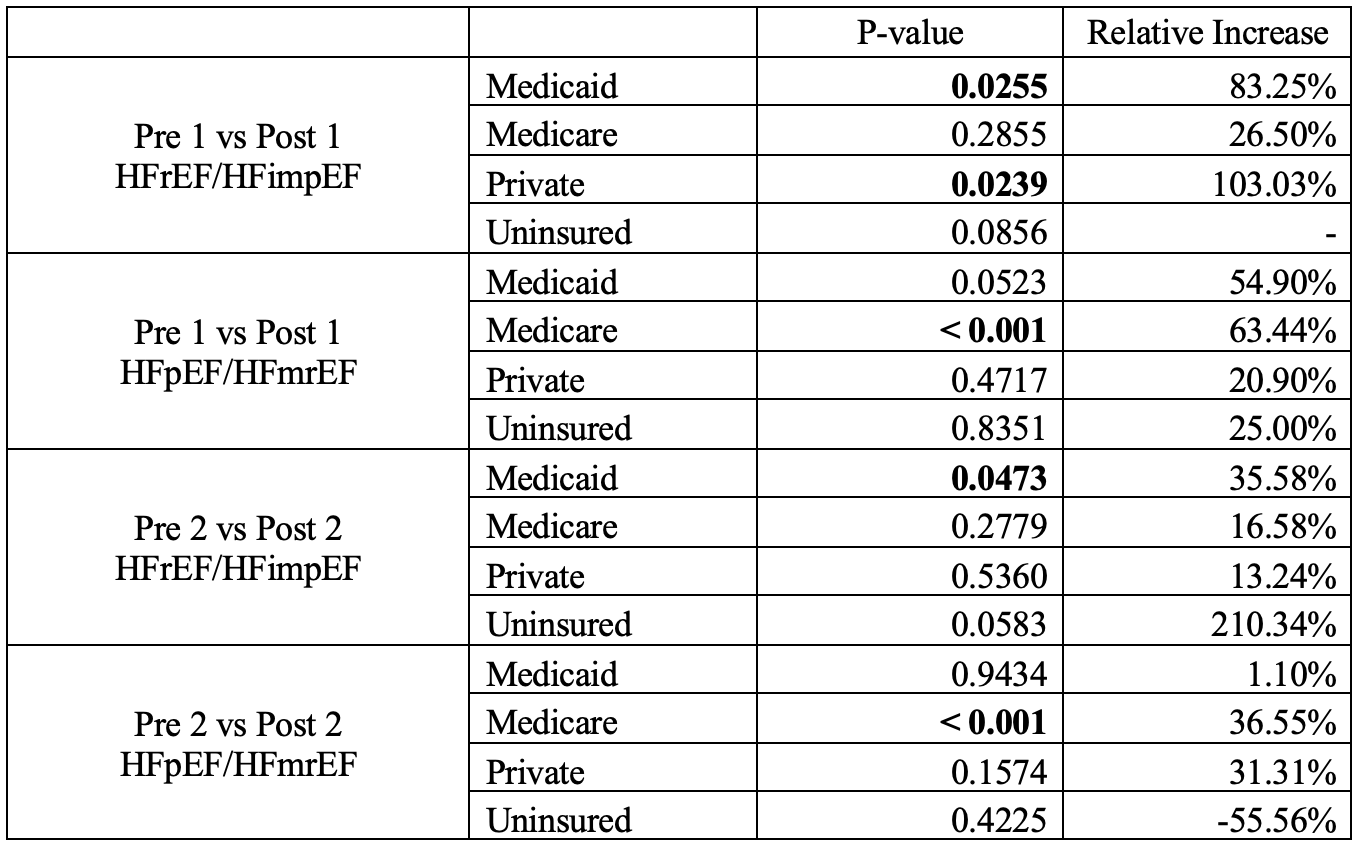
Results: A total of 7,282 patients were analyzed across 11 hospitals. Medicaid saw significant increases in 4-pillar GDMT prescribing in Post 2 and Post 1 but no significant changes in SGTL2is. Medicare saw significant increases in SGLT2i prescribing in Post 2 and Post 1 but no significant change in 4-pillar prescribing. Private insurance saw a significant increase in 4-pillar GDMT prescribing in Post 1 but no significant change in other scenarios. There were no significant changes in prescribing for uninsured patients across any scenario. (Table 1)
Conclusions: Targeted interventions at our hospitals improved GDMT prescribing overall, with the largest gains observed in Medicaid and Medicare patients. These findings highlight differential impacts of interventions across insurance types, suggesting that payer status may influence the effectiveness of quality improvement efforts. Medicaid patients typically face minimal copays ($0-1), which may facilitate obtaining costly therapies in 4-pillar GDMT such as ARNI and SGLT2i. We note, however, there was not an increase in SGLT2i prescribing in patients with Medicaid so there may be an additional confounder. For Medicare, the improvement in SGLT2i prescribing after both interventions may be due to a combination of expanded coverage in Part D and dapagliflozin becoming generic during the study period. Though we expected blunting of effects in uninsured patients, we were disappointed to see no change; we will need to explore effects and interventions including more effective guidance of affordable alternatives (e.g., ACEi/ARB instead of ARNi). Though we generally would expect private insurance to benefit the most, we note a more limited significant effect – perhaps related to outsized co-pay effects as compared to Medicaid. Further research is needed to investigate the mechanisms underlying these disparities to inform the next iteration of our interventions.