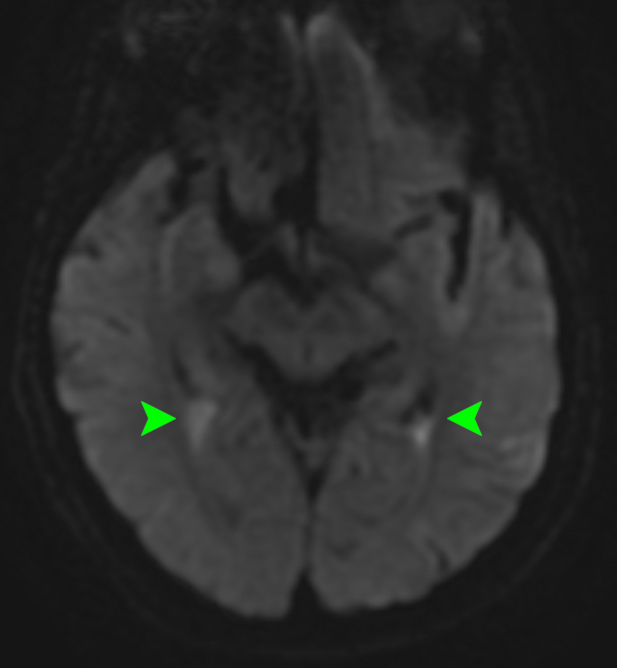
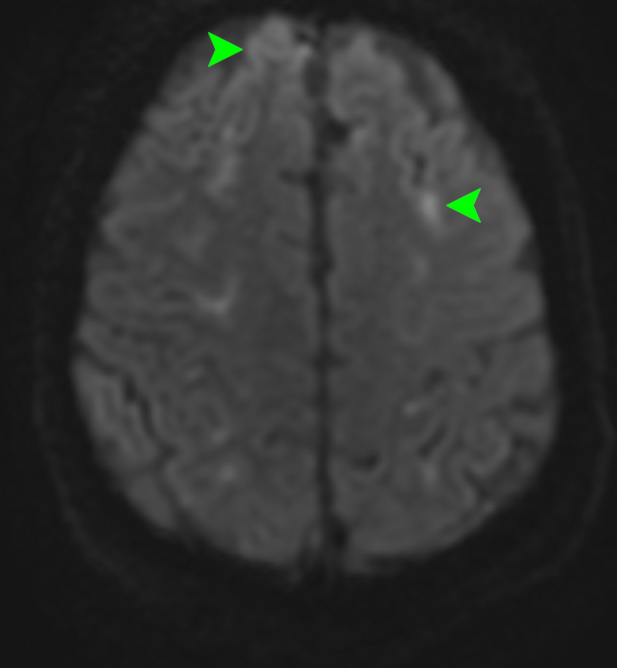
Case Presentation: A 68-year-old male with a pituitary adenoma resected 6 months ago complicated by panhypopituitarism on oral hydrocortisone, presented to the ED with acute progressive altered mental status, headache, and fatigue. On the day of presentation, he became confused to the point where he could not dress himself. Vitals were significant for HR 98. Physical exam was remarkable for confusion, but otherwise nonfocal neurologic exam. CBC showed a WBC of 21.2 K/uL with 79% neutrophils and 18% bands. CT head and CTA head and neck were negative. He became progressively more agitated, and was intubated for airway protection. Lumbar puncture showed glucose of 5 mg/dL, WBC 5500 cells/uL with 98% neutrophils, 2% lymphocytes, and protein 1513 mg/dL. Meningitis PCR panel was positive for Streptococcus pneumoniae, confirmed by CSF culture. He was treated for pneumococcal meningitis with ceftriaxone and 3 days of high dose dexamethasone. He was extubated on day 3, but remained confused. MRI brain demonstrated restricted diffusion at the atria of the lateral ventricles [Image 1] along with sulcal foci of restricted diffusion throughout the frontal and parietal lobes [Image 2], that were concerning for ventriculitis and cerebritis. EEG was negative for seizure. He completed an additional 5 days of methylprednisolone. By day 10, his confusion resolved. He was discharged after completing 14 days of antibiotics.
Discussion: In this case of pneumococcal meningitis, our patient had sustained altered mental status after 3 days of antibiotic therapy and steroids. This led us to obtain an MRI, where we found evidence of ventriculitis and cerebritis. Ventriculitis is thought to be the result of hematogenous spread of bacteria into the choroid plexus. Severe complications can occur with abscess formation or basal cisterns involvement. If untreated, ventricular septations may develop resulting in multiloculated hydrocephalus. CT with contrast may show ependymal enhancement in the ventricles. MRI is most sensitive at detecting ependymal enhancement with T2 hyperintensity and restricted diffusion on DWI, especially in the dependent occipital horns of the lateral ventricles. Cerebritis is the consequence of inflammation in the parenchyma of the brain, which can lead to liquefactive necrosis and abscess formation. CT appears normal in early cerebritis, but MRI may show foci of T1 hyperintensity and restricted diffusion on DWI. Uncomplicated infectious ventriculitis and early cerebritis is treated with antibiotics similar to meningitis. Corticosteroids may be added to prevent neurologic complications. In our case, we extended the course of glucocorticoid in the setting of prolonged confusion. In complicated cases, surgical drainage of an abscess or shunting may be necessary.
Conclusions: Ventriculitis and cerebritis are complications of meningitis, which should be suspected in patients without clinical improvement after initiating appropriate antibiotics. Altered mental status is a common cause of medical admissions and when the differential remains vast, as demonstrated in the case, an MRI can bring clarity and augment diagnosis and treatment.