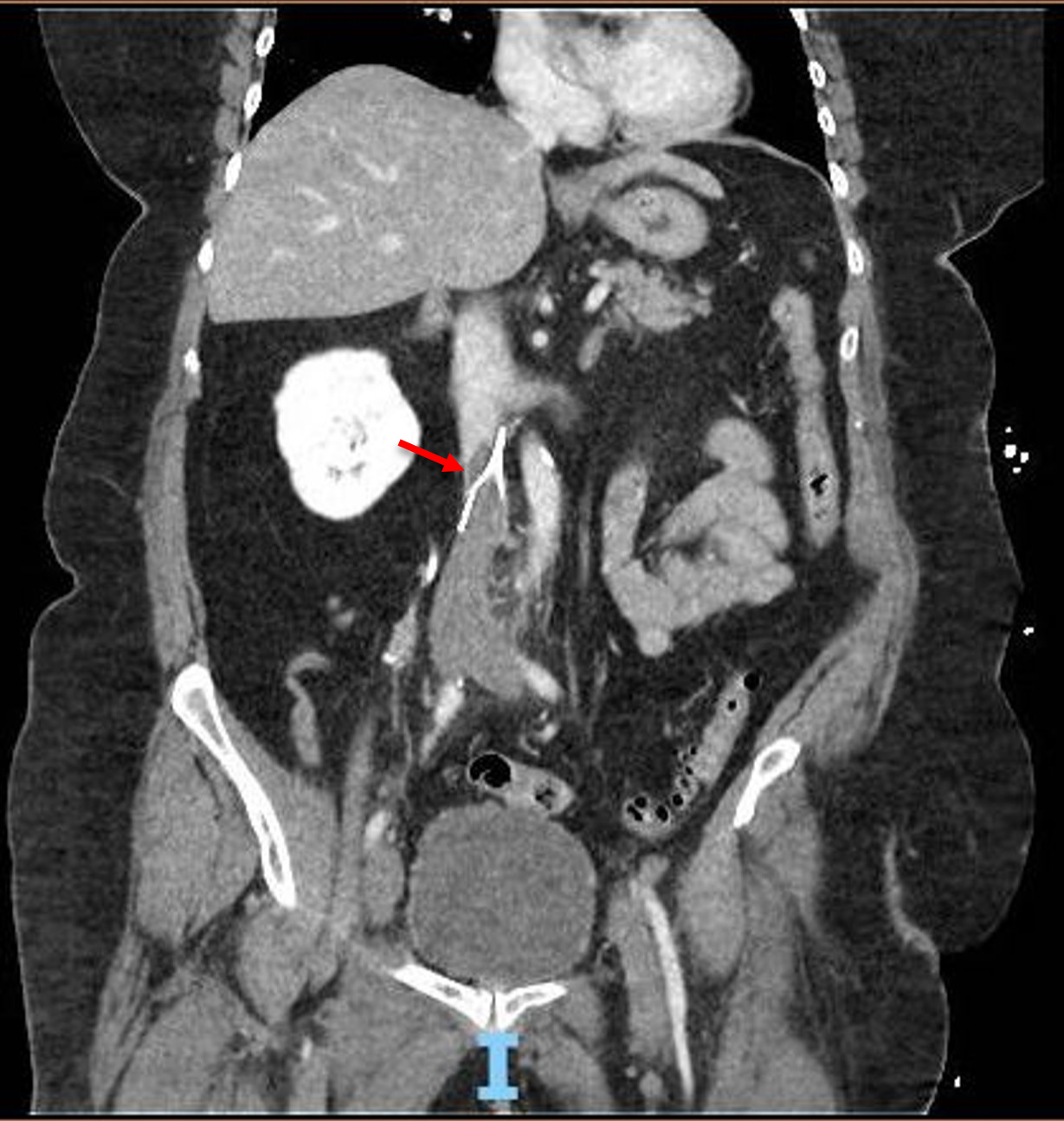
Case Presentation: A 68 year-old female with history of abdominal hysterectomy complicated by post-operative lower extremity deep vein thrombosis (DVT) and prophylactic inferior vena cava (IVC) filter placed prior to past knee replacement surgery now presenting to the hospital with severe right lower extremity pain and swelling impairing her ability to ambulate. On physical exam, patient had pitting edema and diffuse erythema of the right lower extremity. Laboratory values were only notable for leukocytosis. Lower extremity ultrasound revealed extensive, acute, occlusive DVTs of the bilateral popliteal, femoral, and iliac veins as well as all the imaged calf veins. CT angiogram of the abdomen and pelvis showed extensive IVC clot burden with thrombus extending up to and partially beyond the level of the IVC filter. The patient was initially managed with a continuous heparin infusion with partial thromboplastin time (PTT) monitoring and experienced marginal relief of symptoms. The patient was evaluated by vascular surgery and interventional radiology and was offered catheter directed therapy (CDT) due to significant thrombus and symptom burden. She underwent pharmacomechanical thrombectomy and thrombolysis with the Angiojet™ and Penumbra® systems with a large amount of thrombus successfully aspirated. The patient experienced significant relief of symptoms and was able to independently ambulate one day post-procedure. Follow up lower extremity ultrasound three days post-procedure revealed resolution of DVT and the patient was discharged home on oral anticoagulation.
Discussion: Acute deep venous thrombosis is a relatively common diagnosis that is encountered in the inpatient setting. Diagnosis often involves a focused physical exam, ultrasound of the lower extremities and, if warranted, concurrent angiography of the affected vessels. The treatment of DVTs simply involves anticoagulation, often initially with heparin which is then transitioned into an oral regimen upon discharge. Most patients begin to experience symptom relief in a relatively short period after initiation of anticoagulation therapy. Certain factors however, can significantly increase the complexity of the management of DVT. The presence of an IVC filter (which after its intended period of use can be pro-thrombotic) should be addressed and removed if warranted. The utilization of CDT is another therapeutic option that is beginning to see more frequent use. Often CDT is reserved for more life-threatening cases, such as in patients with pulmonary embolism and hemodynamic compromise. However, recent studies have shown that in some cases CDT can improve outcomes, especially in terms of the post-thrombotic syndrome. In this sense, deployment of CDT should be considered on a case by case basis and after extensive discussion with the patient regarding the risks and potential benefits. In a case such as this one, the symptom burden alone can be a major factor in this decision process.
Conclusions: Acute DVTs are a common problem in inpatient medicine with well established guidelines for management. However, many factors exist that can complicate management. Clinicians should be aware of how these factors play into the overall clinical picture and be aware of new and emerging therapeutic options such as CDT that can be incorporated into their shared decision making with patients.