Background: High-need, high-complexity (HNHC) patients experience frequent hospitalizations and drive a disproportionate share of healthcare costs. Fragmented care within large hospital medicine teams may exacerbate these challenges.
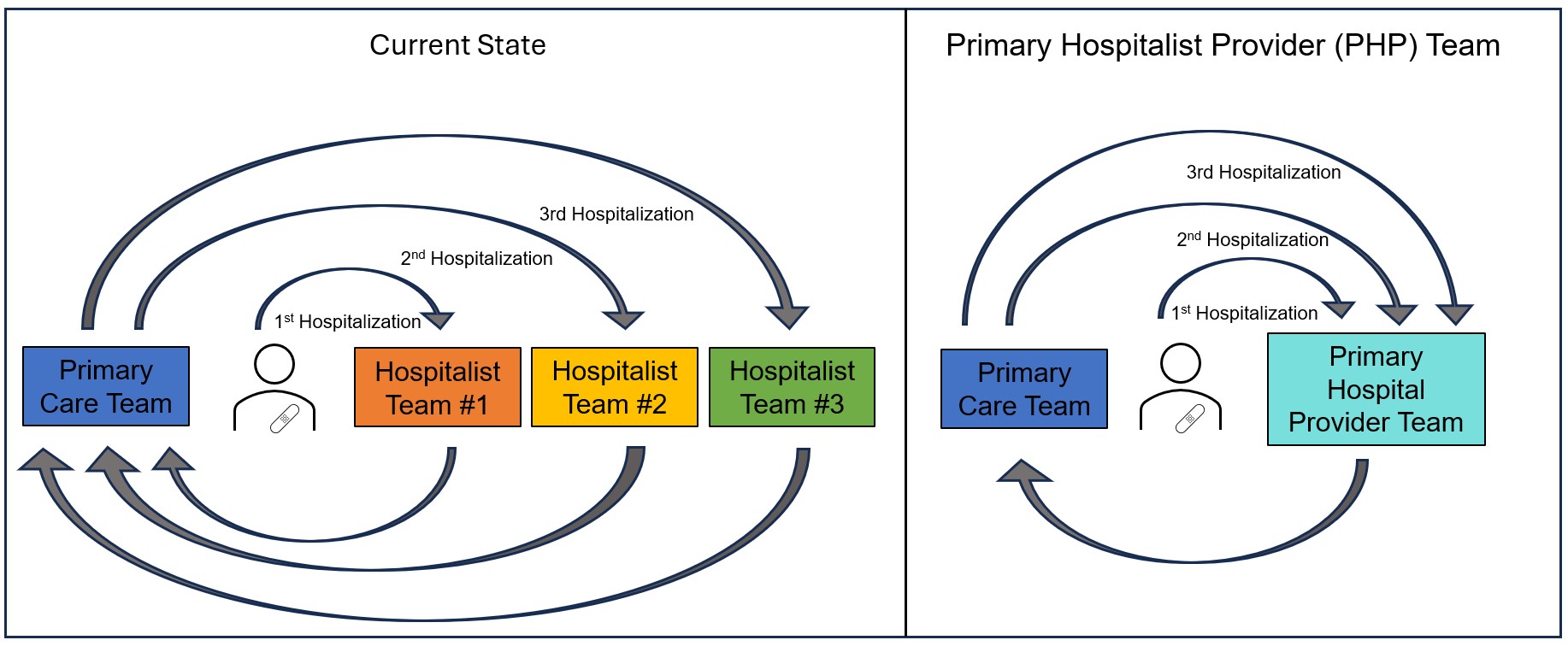
Purpose: To improve inpatient continuity for this vulnerable population, we restructured one hospital medicine team at our academic medical center into a Primary Hospital Provider (PHP) Team.
Description: Our hospital medicine division includes over 80 physicians and 15 advanced practice providers (APPs). We designated a small group—seven physicians and two APPs—to rotate exclusively on the PHP team to enhance continuity for HNHC patients. Physicians self-selected for the team and included four existing hospitalists and three new hires; both APPs were newly recruited for this role.To accommodate scheduling complexities, we partnered with clinical operations leadership to ensure continuous coverage: one physician serves seven consecutive days while APPs alternate in three- to five-day blocks.We collaborated with our hospital’s informatics team to develop a Best Practice Alert identifying eligible patients (greater than 2 hospitalizations in the past 12 months and an Epic Readmission Risk Score above a defined threshold). On subsequent hospitalizations, patients initially assigned to the PHP Team were preferentially reassigned to the PHP Team as census allowed.Additionally, we also recruited a dedicated RN case manager to support care transitions between the inpatient and outpatient setting for our “PHP” patients. To strengthen communication, we instituted weekly virtual meetings to review active PHP patients, address follow-up concerns, and discuss complex cases, social dynamics, and evolving goals of care.
Conclusions: HNHC patients may benefit from improved continuity and care coordination. Establishing such a team requires close collaboration between clinical and operational stakeholders. This model highlights the potential for team-based innovations to reduce fragmentation and improve quality for patients with complex needs. Future work to evaluate the impact of this model on readmissions, patient experience and workforce outcomes is currently underway.